


The worldwide prevalence of myopia has increased over the past few decades, with an emerging epidemic in parts of Asia.1,2 Uncorrected refractive error continues to be a leading cause of visual disability among children globally, and the age of onset for myopia is skewing younger, which allows more time for progression before refractions stabilize.1,2 It is estimated that, by 2050, half of the world’s population will be myopic and 10% will have high myopia.2
AT A GLANCE
- The worldwide prevalence of myopia has increased over the past few decades.
- Studies suggest that both low-dose atropine (0.01%) eye drops and increased time outdoors protect children against the progression of myopia.
- Insufficient scientific evidence currently exists to support interventions such as the purposeful undercorrection of myopia, orthokeratology, and changes in spectacle use.
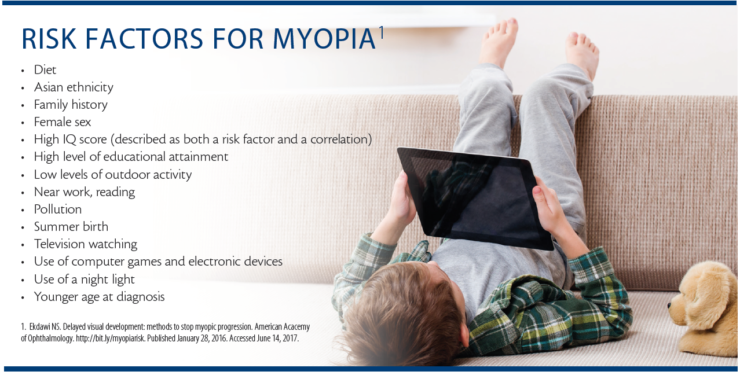
Progressive myopia is especially worrisome because of the increased risk of secondary lacquer cracks, myopic degeneration, posterior staphylomas, retinal detachments, and glaucoma. Although ethnicity and genetics play a role, the rapid increase in myopia’s prevalence is likely driven by environmental factors and modern-day lifestyles, including less time outdoors and more near-based activities than in past generations.
Several modalities to slow the progression of myopia are being investigated. Recent studies have noted some successes, but many challenges remain.
ATROPINE
Although the exact mechanism by which atropine eye drops halt the progression of myopia is not understood, this medical approach is widely used in Taiwan, Singapore, and elsewhere around Asia. In the ATOM 2 (Atropine for the Treatment of Myopia) study, low-dose atropine (0.01%) eye drops effectively slowed myopia progression and had less of a rebound effect when halted compared with higher concentrations. Patients on low-dose therapy described a minimal effect on pupillary size and accommodation and no effect on near visual acuity.3 Based on the ATOM studies, proposed guidelines recommend initiating a 2-year trial of atropine 0.01% in patients between the ages of 6 and 12 whose myopia has increased by more than 0.50 D during the past year.3
Many questions remain regarding who may benefit most from intervention, and long-term follow-up is needed to determine if these changes are permanent.
TIME OUTDOORS
Increasing the amount of time children spend outdoors is a simple and effective preventive option. A recent meta-analysis suggests that an increase of 76 minutes/day of time outdoors may attain a 50% reduction in the incidence of myopia, but further investigation is still needed.4 One assumption is that outdoor activity counters the effect of near work, but time spent outdoors may be an independently protective factor.5 Several hypotheses correlate the role of retinal dopamine release, ultraviolet light exposure, vitamin D, pupillary constriction while outdoors, and/or increased physical activity with the reduction in myopia progression. Most children studied are under 15 years of age. Longer-term studies are needed, but lifestyle modifications and perhaps a change in school policies may be indicated.
OPTICAL INTERVENTIONS
Undercorrection
Not only does the purposeful undercorrection of myopia not prevent its progression, but myopic defocus may actually worsen myopia and increase axial length.6
Contact Lenses
Rigid gas permeable contact lenses may decrease the progression of myopia, but there is a lack of compelling scientific evidence that the effect is long-lived.7 Reverse-geometry–designed contact lenses worn overnight flatten the central cornea and cause the peripheral stroma to swell. Referred to as orthokeratology, this form of treatment theoretically creates an optical blur, which may decrease the elongation of the axial length, but potential complications, including the risk of infectious keratitis, have limited its use.7
Spectacles
The Correction of Myopia Evaluation Trial (COMET) compared the use of progressive/no-line bifocals to single-vision lenses in children with myopia. The researchers found a slight difference in myopia progression but not enough to justify changing the recommendation of how glasses are prescribed.8 That said, in cases of rapidly progressive myopia, prescribing spectacle lenses with a higher add than used in the COMET may be of benefit.
CONCLUSION
Myopia is associated with significant visual disabilities, increased cost, and reduced quality of life, but there is no universally accepted preventive guideline. At this time, low-dose atropine and increased time outdoors are the most promising available treatments. Early intervention is the key to addressing this growing epidemic, but long-term studies are needed before recommendations and changes to practice guidelines can be made.
1. Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2004;33(1):27-33.
2. Holden BA, Fricke TR, Wilson, DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 to 2050. Ophthalmology 2016;123:1036-1042.
3. Chia A, Lu QS, Tan D. Five-year clinical trial on atropine for the treatment of myopia 2: myopia control with atropine 0.01% eyedrops. Ophthalmology. 2016;123:391-399.
4. Xiong S, Sankaridurg P, Naduvilath T, et al. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol. doi:10.1111/aos.13403.
5. Dirani M, Tong L, Gazzard G, et al. Outdoor activity and myopia in Singapore teenage children. Br J Ophthalmol. 2009;93(8):997-1000.
6. Chung K, Mohidin N, O’Leary DJ. Undercorrection of myopia enhances rather than inhibits myopia progression. Vision Res. 2002;42:2555-2559.
7. Van Meter WS, Musch DC, Jacobs DS, et al. Safety of overnight orthokeratology for myopia. Ophthalmology. 2008;115(12):2301-2313.
8. Gwiazda J, Hyman L, Hussein M, et al; the COMET Group. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. IOVS. 2003;44:1492-1500.

