

Not long ago, cataracts in eyes with zonular dialysis or deficiency struck terror in the hearts of cataract surgeons, because these patients were vulnerable to a host of complications, including vitreous loss, dislocation of lens fragments into the posterior segment, and inadequate support for an IOL. Many of these cases ended up in the hands of vitreoretinal surgeons for pars plana vitrectomy and lensectomy with or without sclera-fixated, iris-fixated, or anterior chamber IOLs. How times have changed! Heralded by the introduction of the capsular tension ring (CTR), a wide variety of devices are now available to help cataract surgeons manage these (still) challenging eyes much better (see Supply List for the Maximally Equipped OR).
AT A GLANCE
• The devices to be used during cataract surgery on eyes with zonular instability may be divided into disposable elements for intraoperative stabilization and implants for long-term fixation.
• A complete CCC is critical for the safest execution of phacoemulsification. Iris retractors can provide the necessary stability for creating the tear in eyes with zonular instability.
• Several implantable devices, mainly rings and segments, exist for both capsular expansion and support.
The devices used for eyes with zonular instability may be divided into (1) disposable elements for intraoperative stabilization and (2) implants for long-term fixation. In eyes with zonulopathy or in cases of subluxated IOL-capsular bag complexes, a structurally intact or nearly intact capsular bag is a requirement for the use of these special techniques.
CAPSULORHEXIS
For cataract surgery, a complete continuous curvilinear capsulorhexis (CCC) is critical for the safest execution of phacoemulsification. Puncturing the anterior capsule can be especially challenging when the zonules are weak or absent, because directing a cystotome posteriorly may be met with no countertraction and simply displace the lens. The use of two apposing 30-gauge needles to tangentially pinch the anterior capsule between the opposing tips will guarantee penetration through the capsule by one needle or the other. Sometimes, the capsulorhexis can be peeled in the usual fashion. In many zonulopathy cases, however, circumferential countertraction is absent, and propagation of the capsulorhexis tear is very difficult. Placing a small, flexible iris retractor through a small paracentesis into the initial tear can stabilize the lens enough for the surgeon to continue the CCC. It is important not to try to recenter the lens with this device or to tighten the retractor too much, because such a maneuver could cause the CCC tear to extend equatorially. Sequential placement of additional iris retractors as the tear proceeds can be very useful for profound zonular damage.
THE CAPSULAR BAG
Some surgeons use flexible iris retractors throughout phacoemulsification to stabilize the capsular bag. Although these hooks work well in many cases, it is important to remember that the hooks stabilize the bag at the CCC margin, not at the bag’s equator. Accordingly, the equator can still be aspirated inadvertently during phacoemulsification or cortical removal. Also, the sharper edges of the hook can rarely cause the capsular margin to break. In contrast, capsule hooks are designed with either a round ball on the end or a double-looped hook, the smooth end of which can support the capsule at the equator and strongly stabilize the bag during the case without risk to the CCC margin (Figure 1). Unfortunately, these retractors are a little bigger and bulkier than the more slender iris retractors and, thus, cannot be safely placed until the CCC has been completed. During a CTR’s insertion into the bag, a potential pitfall is unknowingly threading the ring through the loop of the hook in the bag’s equator. This can obviously make removal of the retractor at the conclusion of phacoemulsification both unsafe and ineffective.
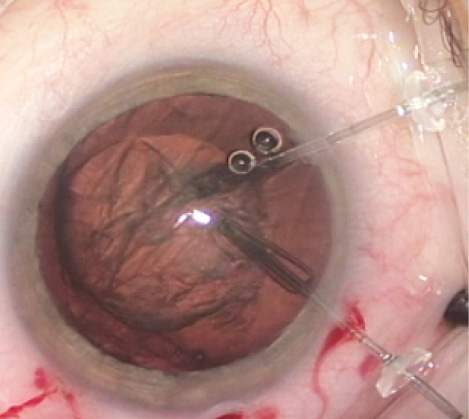
Figure 1. The looped ends of two capsule retractors (MicroSurgical Technology) support the equator of the capsular bag rather than the capsulorhexis margin. These hooks are larger than iris retractors, though, and thus consume more of the central working space than iris hooks, which “tent” the CCC margin.
Several implantable devices exist for both capsular expansion and support. A standard CTR threaded into the fornix of the capsular bag fully expands a flaccid bag and uniformly distributes the support of the remaining zonules to the entire bag complex. This strategy works well in cases of mild to moderate dialysis when the integrity of the remaining zonules is sound. It is also an excellent option for patients with conditions associated with known progressive zonulopathies like pseudoexfoliation and retinitis pigmentosa but who do not yet have weakness. If a capsular bag becomes loose in the future and an indwelling CTR is in situ, repositioning and suture fixation are easier, safer, and faster than repositioning or exchanging a lens implant in a flaccid bag with no CTR in place. A Henderson CTR (Morcher, distributed in the United States by FCI Ophthalmics) is similar to a standard CTR, but the former’s periodic cog-like undulations are designed to prevent the entrapment of cortical fibers if the device is placed prior to cortical removal. The Henderson CTR can also be very useful in cases of toric IOLs when there is an oval capsular bag or an otherwise high risk of IOL rotation. The cogs in the Henderson CTR will lock the haptics of the toric IOL in place.
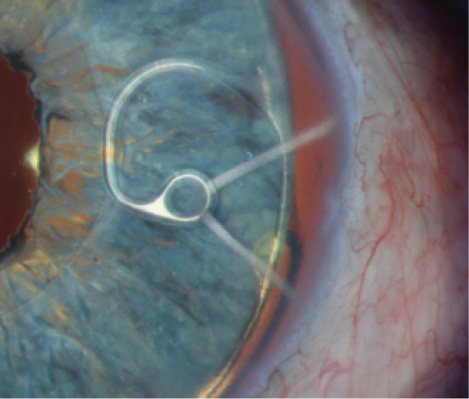
Figure 2. A slit-lamp photograph shows the fixation element of a Cionni Ring for Scleral Fixation in situ within the capsular bag in front of a customized iris prosthesis. The CTR and IOL haptic’s edge can be seen in the equator of the bag.
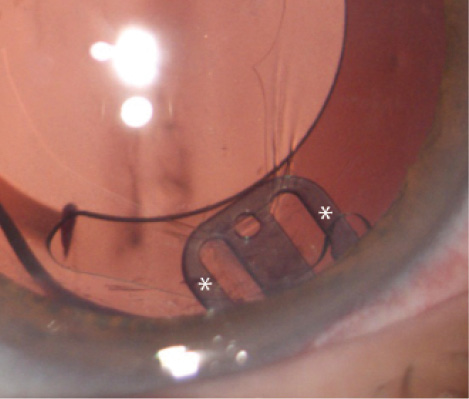
Figure 3. The AssiAnchor in situ. Two arms with asterisks are within the capsular bag; they support the equator and the CCC margin. The central component of the device extends anterior to the capsule, where it abuts the internal eye wall at the ciliary sulcus.
SUPPLY LIST FOR THE MAXIMALLY EQUIPPED OR
• 30-gauge needles
• flexible iris retractors
• capsule hooks
• capsular tension rings
• Henderson Capsular Tension Ringsa
• Cionni Rings for Scleral Fixationa
• Ahmed Capsular Tension Segmentsa
• AssiAnchorb
aManufactured by Morcher and distributed in the United States by FCI Ophthalmics.
bManufactured by Hanita Lenses, not available in the United States.
For cases in which existing zonular support is inadequate for bag centration or stabilization, a CTR that can be fixated is a preferable option. The Cionni Ring for Scleral Fixation (Morcher, distributed in the United States by FCI Ophthalmics) has a fixation element that courses around the CCC margin from the ring into the anterior chamber. The surgeon can place a suture through this fixation element to suspend the device from the scleral wall (Figure 2). This CTR can provide significant structural stability to the bag and fixate it well to the scleral wall, but it takes some dexterity on the part of the surgeon to place the device completely within the capsular bag. A Malyugin Ring (MicroSurgical Technology) has the fixation element on the leading edge of the ring and, therefore, can be placed via an injector system. Although this design is preferable in some ways, it does not provide as broad a range of contact of the fixation point with the capsular bag. It can be challenging to place a CTR of any type in the bag when nuclear or cortical material is still present.
The Ahmed Capsular Tension Segment (Ahmed CTS; Morcher, distributed in the United States by FCI Ophthalmics) is a 120º arc of a CTR. The Ahmed CTS has a fixation element similar to that of the Cionni Ring. The segment can be used early in surgery for temporary stabilization, supported by an iris hook, and as a permanently implantable device. An Ahmed CTS can be more easily placed than the Cionni Ring because of its smaller size, but the surgeon must be careful not to overtighten the fixation element of a segment. The device is retained only by the anterior capsular leaflet, and the torque by overtightening can cause the Ahmed CTS to pop out of the bag’s equator. This problem does not occur with the suture-fixated CTRs, because the opposing zonules create countertraction to the induced torque. Greg Ogawa, MD, recently introduced a modification of the CTS that has the fixation eyelet closer to the outer perimeter of the segment than that of the original Ahmed 6D and 6E devices and has more anteriorly curved ends to the segment, which may help reduce torque in comparison to the current iteration (information available from Morcher).
Watch it Now
Michael E. Snyder, MD, demonstrates phacoemulsification combined with vitrectomy for a profoundly loose lens with vitreous in the anterior chamber from the start.
When trying to refixate an existing, newly subluxated bag-IOL complex, it is rare that the entire capsular bag can be opened, making the placement of a Cionni Ring difficult. It is often possible, however, to open some (but not all) bags for the requisite 4 clock hours to sneak in an Ahmed CTS.
CONCLUSION
With the advent of innovative temporary and permanently implanted devices, the loose lens and loose IOL have become less vexing and management more facile. More options are on the horizon. Although not yet available in the United States, the AssiAnchor (Hanita Lenses) is a small, flat PMMA device that functions much like a paper clip by supporting the equator of the bag and folding anterior to the CCC (Figure 3). The device’s fixation aperture is peripheral to the equator of the capsular bag, so minimal to no torque is induced. Although the AssiAnchor can be used to stabilize a capsular bag at the time of cataract surgery, it may also be more amenable than an Ahmed CTS for refixation of a bag-IOL complex with late zonulopathy, because its narrower profile requires only a 2.5-mm area of the capsular bag to be opened rather than a 120º arc.
Michael E. Snyder, MD
• member, Board of Directors, Cincinnati Eye Institute
• volunteer faculty, University of Cincinnati
• (513) 984-5133; msnyder@cincinnatieye.com
• financial disclosure: consultant to HumanOptics, manufacturer of the custom iris device depicted in Figure 2

