



Corneal cross-linking (CXL) has established a new paradigm for the treatment of progressive ectasia and keratoconus.1,2 The visual rehabilitation of patients who achieve stability after CXL can be challenging if they were intolerant of rigid gas permeable contact lenses or if they had poor vision with glasses and/or soft contact lenses prior to treatment. The problem led my colleagues and me to introduce the topography-guided normalization of corneas that remain highly irregular despite some flattening effect from CXL.3,4
EARLY EFFORTS
At the outset, we waited at least 6 months after CXL to perform topography-guided partial PRK. Because these were “uncharted waters,” we set an arbitrary 50-µm limit to the ablation over the cone. Admittedly, such conservative treatment did little to correct refractive error.5-12
AT A GLANCE
- To promote visual rehabilitation, the author and his colleagues introduced the topography-guided normalization of corneas that remain highly irregular despite some flattening effect from corneal cross-linking.
- Sequential treatment involves performing cross-linking first and topography-guided partial PRK at least 6 months later. In the combined approach, also termed the “Athens protocol,” the two procedures are performed on the same day.
We decided that, if the corneal parameters permitted, we would treat up to 70% of the sphere and cylinder but always maintain that 50-µm maximum ablation over the thinnest part of the cone. The refractive effects of this treatment strategy were impressive: the great majority of patients obtained a BCVA of 20/40. Few complications occurred aside from some PRK-related haze and occasionally delayed epithelial healing.13 We therefore began to discuss our findings with prospective CXL patients and to offer them the option of CXL and partial topography-guided PRK as a combined, same-day procedure.
ADVANTAGES
Our early experience identified three advantages of our combined approach. First, there is no need to remove cross-linked cornea (the CXL effect is greater closer to the surface). With a sequential approach, surface ablation removes some of the most biomechanically stable corneal tissue produced by CXL.12
Second, we observed less corneal haze and scarring in these eyes.12 A third and surprising finding was that performing CXL and topography-guided PRK at the same time had a synergistic effect: we achieved greater corneal flattening and a more dramatic refractive effect (see A Clinical Example below).12
A Clinical Example
A 23-year-old man had progressive keratoconus in his right eye. In 2008, his refraction was -5.00 -3.00 × 130, and his BSCVA measured 20/60. The patient underwent treatment using the Athens protocol in 2009: topography-guided PRK -2.00 -1.50 × 121 (the topography axis) combined with same-day corneal collagen cross-linking.
Eight years later, his keratoconus is stable, and the patient has a distance UCVA of 20/25. His refraction is currently +0.50 -100 × 050 = 20/20 (Figure).
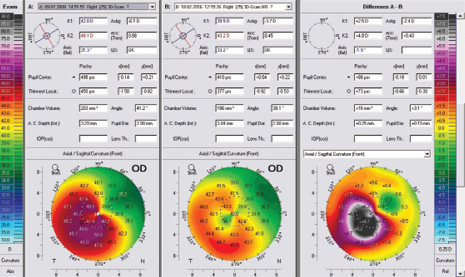
Figure. Preoperative measurements (left). Eight years postoperatively (middle). The difference between the pre- and postoperative measurements (right) demonstrates the high degree of treatment accuracy and remarkable flattening of almost 9.00 D at the peak of the cone.
RESULTS AND REFINEMENT
We carefully studied our results in approximately 200 procedures of CXL first and topography-guided partial PRK performed 6 months later at the earliest, and we compared them to the results of more than 200 cases in which CXL and PRK were performed simultaneously.12 We named the combined same-day procedure the “Athens Protocol” and have since reported on over 1,000 cases, both primary keratoconus and post-LASIK ectasia, and their long-term follow-up.5-12
We have since enhanced the Athens protocol. Because the epithelium of these eyes is invariably highly irregular, we remove the tissue via phototherapeutic keratectomy using a 7-mm optical zone and a depth of 50 µm. We use the epithelium as a “masking agent” for the topography-guided PRK procedure.
Another change we have made is a transition to higher-fluence ultraviolet light for CXL: 6 mW/cm2 applied for 15 minutes for the same total energy of 5.4 J.5 Moreover, like most investigators globally, we use riboflavin solution based in saline rather than dextran for better absorption and less dehydration of the stroma.12
COMBINED VERSUS SEQUENTIAL TREATMENT
The argument against the combined procedure is as follows: one cannot predict the long-term refractive effects of CXL,13 so it is not possible to predict what the refractive error produced by the combination technique will be. We have indeed observed a few cases of a slight refractive overcorrection after more than 10 years of follow-up, when the postoperative refraction was initially on target for the first couple of years. Another significant concern regarding the Athens protocol is the combined ultraviolet assault on the epithelium from PRK and CXL, with delayed epithelial healing and stromal loss as potential sequelae.13
Sequential treatment is certainly a valid option. After performing CXL, the ophthalmologist monitors the patient’s visual rehabilitation and considers the possibility of contact lenses or a phakic IOL if anisometropia or residual refractive error persists. If needed, the surgeon performs a partial topography-guided PRK 6 months or longer after CXL, when most of the healing has taken place. Again, the disadvantage is that PRK will remove some of the most biomechanically stable tissue produced by the CXL procedure.
The combined approach reduces patient morbidity. In our experience, it is also far more attractive to patients. Proper informed consent is needed so they understand that the Athens protocol cannot be a fully predictable refractive procedure—not comparable to today’s routine PRK and LASIK.9,12,14,15 Further visual rehabilitation with soft contact lenses, glasses, or potentially a future refractive procedure on the cornea or with a phakic IOL may be required if emmetropia or a result approaching it is desired.
Our preference is to inform patients about both options, share with them our experience and clinical outcomes, and let them decide (see video below). To promote a well-educated and thoroughly discussed decision, we ask the family to be present, because most of our candidates are teenaged boys or young adult men (early twenties).
A. John Kanellopoulos, MD, shares two preoperative discussions with patients.
CONCLUSION
The big lesson we have drawn from our extensive study of corneal diagnostics is that not everything that looks like ectasia or keratoconus progression on topography or tomography is what it seems.16,17 A multifactorial assessment of the cornea is necessary to remove bias for potential epithelial remodeling, the use of contact lenses, etc.18-20
As far as combining CXL with partial PRK or performing the procedures sequentially, once surgeons acquire experience with both approaches, they will determine what best meets their patients’ needs.
1. Barbarino SC, Papakostas AD, Sperber L, et al. Post-LASIK ectasia: stabilization and effective management with riboflavin/ultraviolet A-induced collagen cross-linking. Invest Ophthalmol Vis Sci. 2006;47:e-abstract 536.
2. Hafezi F, Kanellopoulos AJ, Wiltfang R, Seiler T. Corneal collagen crosslinking with riboflavin and ultraviolet A to treat induced keratectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2007;33:2035-2040.
3. Kanellopoulos AJ. Post-LASIK ectasia. Ophthalmology. 2007;114(6):1230.
4. Kanellopoulos AJ. An alternative treatment for keratoconus. Cataract & Refractive Surgery Today. January 2007;7(1):70-73. http://crstoday.com/articles/2007-jan/crst0107_09-php/?single=true. Accessed June 21, 2017.
5. Kanellopoulos AJ. Long-term results of a prospective randomized bilateral eye comparison trial of higher fluence, shorter duration ultraviolet A radiation, and riboflavin collagen cross linking for progressive keratoconus. Clin Ophthalmol. 2012;6:97-101.
6. Kanellopoulos AJ, Loukas YL, Asimellis G. Cross-linking biomechanical effect in human corneas by same energy, different UV-A fluence: an enzymatic digestion comparative evaluation. Cornea. 2016;35(4):557-561.
7. Kanellopoulos AJ. Sequential versus simultaneous CXL and topography-guided PRK. CRST Europe. http://crstodayeurope.com/articles/2009-apr/0409_11-php. April 2009. Accessed June 21, 2017.
8. Kanellopoulos AJ, Asimellis G. Comparison of Placido disc and Scheimpflug image derived topography-guided excimer laser surface normalization combined with higher fluence CXL: the Athens Protocol, in progressive keratoconus. Clin Ophthalmol. 2013;7:1385-1396.
9. Kanellopoulos AJ, Binder PS. Management of corneal ectasia after LASIK with combined, same-day, topography-guided partial transepithelial PRK and collagen cross-linking: The Athens Protocol. J Refract Surg. 2011;27(5):323-331.
10. Kanellopoulos AJ, Asimellis G. Keratoconus management: long-term stability of topography-guided normalization combined with high-fluence CXL stabilization (The Athens Protocol). J Refract Surg. 2014;30(2):88-92.
11. Krueger RP, Kanellopoulos AJ. Stability of simultaneous topography-guided photorefractive keratectomy and riboflavin/UVA cross-linking for progressive keratoconus: case reports. J Refract Surg. 2010;26(10):S827-832.
12. Kanellopoulos AJ. Comparison of sequential vs same-day simultaneous collagen cross-linking and topography-guided PRK for treatment of keratoconus. J Refract Surg. 2009;25(9):S812-818.
13. Kanellopoulos AJ, Cho M. Complications with the use of collagen cross-linking. In: Agarwal A, Jacobs S, eds. Complications in Ocular Surgery. Thorofare, NJ: Slack; 2012;115-120.
14. Kanellopoulos AJ, Asimellis G. Epithelial remodelling after partial topography-guided normalization and high-fluence short-duration crosslinking (Athens Protocol); results up to 1 year. J Cataract Refract Surg. 2014;40:1597-1602.
15. Kanellopoulos AJ, Skouteris V. Secondary ectasia due to forceps injury at childbirth: management with combined topography-guided partial PRK and collagen cross-linking (Athens Protocol) and subsequent phakic IOL implantation. J Refract Surg. 2011;27(9):635-636.
16. Kanellopoulos AJ, Krueger R, Asimellis G. Cross-linking and corneal imaging advances. Biomed Res Int. 2015;2015:306439.
17. Kanellopoulos AJ, Asimellis G. Introduction of quantitative and qualitative cornea optical coherence tomography findings induced by collagen cross-linking for keratoconus: a novel effect measurement benchmark. Clin Ophthalmol. 2013;7:329-335.
18. Kanellopoulos AJ, Moustou V, Asimellis G. Evaluation of visual acuity, pachymetry and anterior-surface irregularity in keratoconus and crosslinking intervention follow-up in 737 cases. J Kerat Ect Cor Dis. 2013;2(3):95-103.
19. Kanellopoulos AJ, Asimellis G. OCT corneal epithelial topographic asymmetry as a sensitive diagnostic tool for early and advancing keratoconus. Clin Ophthalmol. 2014;8:2277-2287.
20. Kanellopoulos AJ, Asimellis G. OCT-derived comparison of corneal thickness distribution and asymmetry differences between normal and keratoconic eyes. Cornea. 2014;33(12):1274-1281.

