


Trauma is the most common cause of unilateral cataract in young patients (Figure). At the time of presentation after trauma to the eye, a primary repair of a corneal, iris, or scleral wound may be needed along with a complete evaluation of damage to the intraocular structures (eg, posterior capsular rupture, vitreous hemorrhage, and retinal detachment).
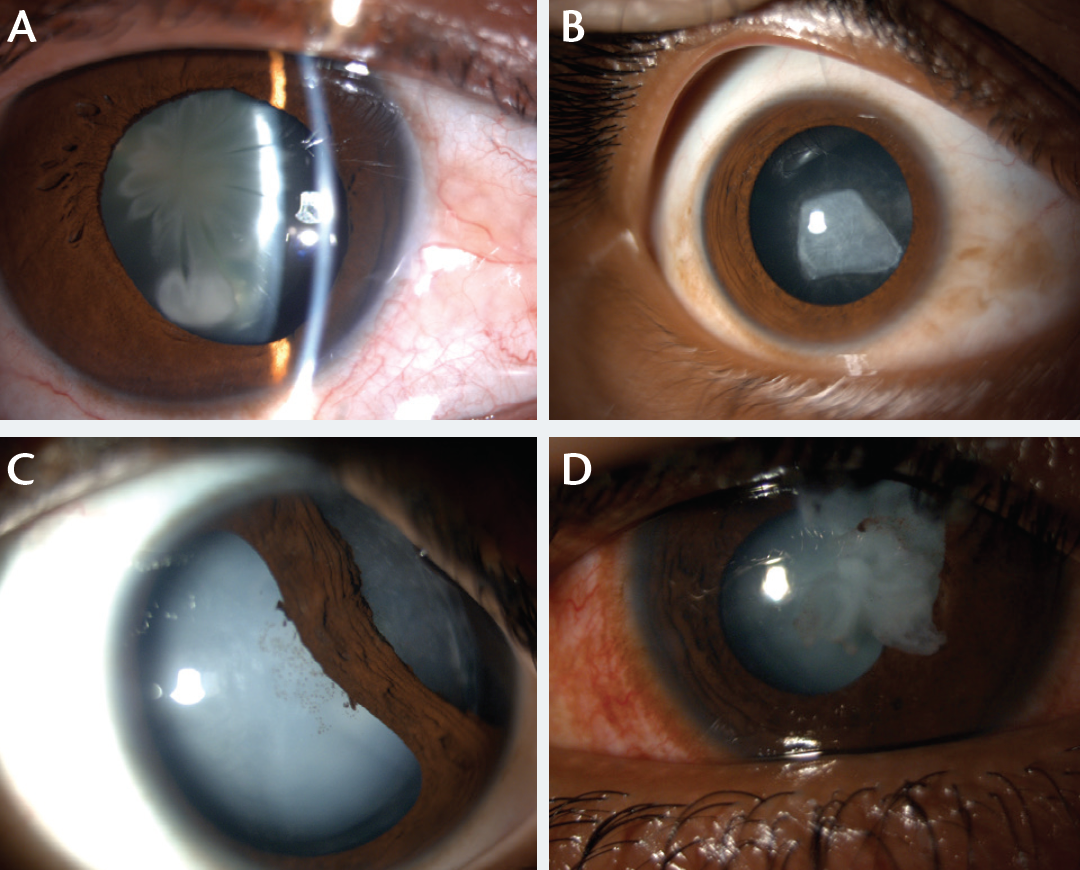
Figure. Ocular trauma is a common cause of unilateral cataract in adults and children (A-D).
We prefer to defer cataract surgery and IOL implantation in cases of traumatic cataract, even when the anterior lens capsule has ruptured. A delay of 3 to 4 weeks may allow corneal healing and reduce the inflammatory response. Longer postponement is avoided in children within the amblyopic age range. IOL implantation is preferred in cases of traumatic cataract with corneal injury. Placement of the IOL’s haptics in the capsular bag is preferred when capsular support is available. Ciliary sulcus fixation of the IOL can also be performed in the absence of adequate capsular support for in-the-bag placement, but it may be associated with a greater incidence of uveitis and pupillary capture. Sutureless scleral fixation of a posterior chamber IOL or iris fixation of an IOL can be performed in the absence of capsular support.
Intracameral antibiotics (0.1 mL Vigamox [moxifloxacin; Alcon]) may help decrease the risk of postoperative endophthalmitis. Preservative-free triamcinolone acetonide (0. 1 mL Aurocort [Aurolab; not available in the United States]) may help to stain the vitreous and decrease postoperative inflammation in traumatic cataract cases.
To watch a video of pearls for premium IOL implantation in eyes with compromised capsular integrity, visit www.youtube.com/watch?v=Nc6FBFuKpMY.
MANAGING TRAUMATIC CATARACT CASES
Case No. 1
A 30-year-old patient presented with a traumatic cataract from a thorn injury to the right eye sustained 5 years earlier. The surgeon faced several challenges: a small irregular pupil that failed to dilate (due to iridolenticular adhesions), a localized calcified cataract, and the presence of posterior capsular plaque. The patient was counseled about the surgical procedure and visual outcome. Topical phacoemulsification (supplemented with preservative-free intracameral lignocaine) and IOL implantation were performed. The corneal endothelium was coated with a dispersive ophthalmic viscosurgical device (OVD; Viscoat [Alcon]). The surgeon stained the anterior capsule and released iridolenticular synechiae with a blunt spatula.
These steps were followed by an anterior capsulorhexis. The soft lens matter was aspirated using low phaco power and fluidics parameters. The calcified capsule/lens matter was removed, and posterior capsular plaque peeling was also performed. A foldable hydrophobic IOL (Care Group; not available in the United States) was implanted in the capsular bag. Preservative-free triamcinolone acetonide and moxifloxacin (0.1 mL) were administered intracemerally. The patient’s BCVA 1 week postoperatively was 20/30.
Case No. 2
A 12-year-old with a traumatic cataract was referred to SuVi Eye Institute, Kota, India, for management. This child had sustained an injury to the right eye 1 month earlier from the thorn of a Babul (Acacia arabica) tree while playing cricket. The patient noticed a gradual decrease in vision in that eye. On examination, there was a corneal scar (inferotemporal region) and a total traumatic white cataract with a torn anterior capsule (horizontal anterior capsular split from the 3- to the 9-o’clock position). B-scan revealed an intact posterior capsule. The patient’s preoperative visual acuity was hand motion close to face (accurate projection of rays in all quadrants), and the IOP measured 18 mm Hg. The parents were keen on having an IOL implanted to minimize the patient’s dependency on glasses. The preoperative keratometry reading showed corneal astigmatism of 0.50 D.
Watch it Now
Drs. Pandey and Sharma demonstrate phacoemulsification in a case of traumatic cataract.

After detailed counseling and an explanation of all relevant details of surgical technique and visual outcome, we selected a Tecnis Multifocal IOL (Abbott Medical Optics) for implantation. We prefer to perform pediatric cataract surgery under general anesthesia, but this case was performed under topical anesthesia. After making the side port incision, we stained the anterior capsule with trypan blue dye under an air bubble and coated the corneal endothelium with a dispersive OVD (Viscoat). An anterior capsulorhexis was not attempted due to the presence of a horizontal anterior capsular split. Soft lens matter was carefully removed using bimanual I/A. The IOL was loaded in the cartridge, and the haptics of the multifocal IOL were carefully positioned at the 6- and 12-o’clock positions of intact capsular fornices. The OVD was removed from behind the IOL. The clear corneal incisions (main and sideports) were sealed. Intracameral self-preserved moxifloxacin and preservative-free triamcinolone acetonide were injected into the anterior chamber.
On postoperative day 1, the multifocal IOL was well centered with minimal inflammation in the anterior chamber. The child regained a UCVA of 20/20 and N5 (unaided).
CONCLUSION
The management of traumatic cataracts can be challenging. The chance of a successful outcome has increased thanks to advanced phaco/vitrectomy machines with improved fluidic parameters, refined surgical techniques, and the availability of various capsular dyes (eg, trypan blue), anti-inflammatory/vitreous staining adjuncts (preservative-free triamcinolone), devices (OVDs, iris hooks, Malyugin Rings [MicroSurgical Technology], capsular tension rings, Ahmed Capsular Tension Segments [Morcher; distributed in the United States by FCI Ophthalmics]), and IOLs (glued IOL/retro-iris fixated). The ophthalmologist’s understanding and thorough evaluation (anterior and posterior segment examination and imaging studies to rule out an intraocular foreign body) of the nature and extent of the ocular damage in addition to careful planning and counseling prior to surgery are imperative to the proper management of these challenging cases.
Suggested Reading
Wilson ME, Trivedi RH, Pandey SK. Pediatric Cataract Surgery: Technique, Complications and Management. Philadelphia: Lippincott Williams & Wilkins; 2005.
Pandey SK, Ram J, Werner L, et al. Visual results and postoperative complications of capsular bag versus sulcus fixation of posterior chamber intraocular lenses for traumatic cataract in children. J Cataract Refract Surg. 1999;25:1576-1584.
Pandey SK, Wilson ME, Trivedi RH, et al. Pediatric cataract surgery and intraocular lens implantation: current techniques, complications, and management. Int Ophthalmol Clin. 2001;41(3):175-196.
Pandey SK, Billson FA. Pediatric Cataract Surgery. Jaypee Brothers: New Delhi, India; 2005.
Ram J, Pandey SK, Apple DJ, et al. Effect of in-the-bag intraocular lens fixation on the prevention of posterior capsule opacification. J Cataract Refract Surg. 2001;27:1039-1046.
Suresh K. Pandey, MBBS, MS
• director at SuVi Eye Institute & LASIK Laser Centre, Kota, Rajasthan, India
• visiting assistant professor at John A. Moran Eye Center University of Utah, Salt Lake City
• visiting surgeon at the Sydney Eye Hospital, Save Sight Institute, University of Sydney, Australia
• +91 93514 12449; suresh.pandey@gmail.com
• financial interest: none acknowledged
Vidushi Sharma, MD, FRCS
• director at SuVi Eye Institute & LASIK Laser Centre, Kota, Rajasthan, India
• +91 93514 12449; suvieye@gmail.com
• financial interest: none acknowledged

