

Each has its place.
By J. David Stephens, MD

Creating a round, centered anterior capsulotomy is arguably the most important step in cataract surgery. Without it, refractive outcomes can be unpredictable owing to variability in the effective lens position and IOL tilt and decentration. If a tear in the posterior capsule occurs, a round, centered capsulotomy allows an IOL to be implanted in the sulcus, and optic capture may be performed to increase lens stability.
New technologies have automated the anterior capsulotomy. Debate continues regarding their utility and cost-effectiveness compared to a traditional continuous curvilinear capsulorhexis (CCC). This article discusses three methods of capsulotomy creation and their roles in modern cataract surgery.
THE MANUAL CCC
The manual CCC has been the preferred technique since the 1990s.1 Advances in intraocular instruments have made the technique reproducible and consistent. I favor the use of capsulorhexis forceps because they open in the eye rather than the incision, cause little OVD egress, and fit through a paracentesis if necessary. Intraocular measuring marks on the forceps facilitate accurate capsulotomy sizing (Figure 1).

Figure 1. A CCC is created with intraocular forceps (MicroSurgical Technologies). Note the measurement markings on the forceps.
Benefits. The manual CCC is fast and inexpensive and may be executed in virtually any eye, including those requiring the use of a pupillary expansion device. Zonular strength can be tested with this technique before nuclear disassembly begins.
Drawbacks. The shape and size of a manual CCC can vary significantly.2 In an eye with a white intumescent cataract, radial elements in the capsule may incite an anterior capsular tear or lead to the Argentinian flag sign. The capsulotomy must be centered visually, typically by using the iris and Purkinje images as points of reference. This may lead to asymmetric or incomplete capsular overlap of the IOL.
LASER CAPSULOTOMY
Benefits. During laser cataract surgery, pulses of energy create a perfectly round capsulotomy that may be centered on the optical or pupillary axis of the eye (Figure 2). The size and location of the capsulotomy may be adjusted precisely based on surgeon preference.

Figure 2. An intraocular view of the laser capsulotomy after nuclear fragmentation.
I use the Ally Adaptive Cataract Treatment System (Lensar), which marks the steep axis of astigmatism on the capsule with small capsular tags.3 Iris registration is loaded directly from the biometer (IOLMaster 700, Carl Zeiss Meditec). Marking the axis on the capsulotomy helps account for cyclotorsion of the eye while the patient is supine and makes toric IOL alignment faster and more straightforward.
The nucleus may also be disassembled and softened during laser cataract surgery, and laser arcuate incisions may be made to treat low levels of astigmatism.
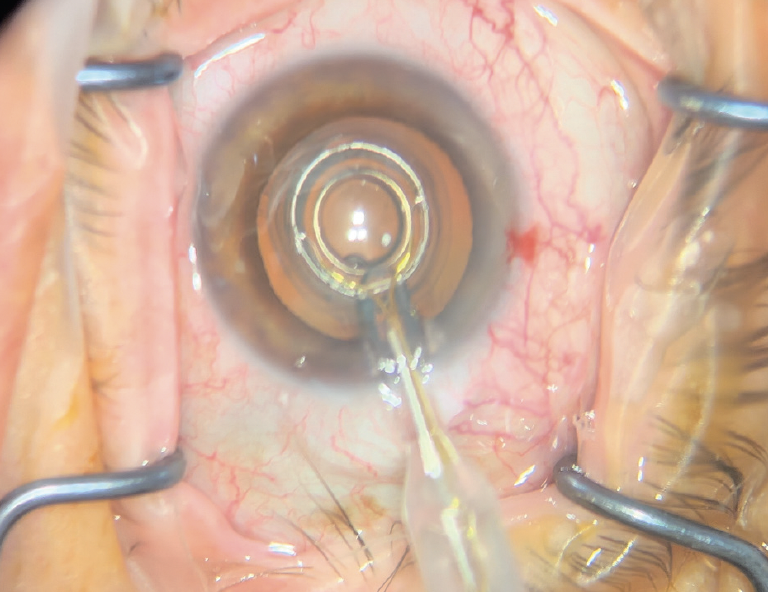
Figure 3. A precision pulse capsulotomy is performed with the Zepto IOL Positioning System.
Drawbacks. The laser system is expensive to purchase or lease. Laser cataract surgery also adds a step to the surgical procedure, which may decrease efficiency. Treatment and docking times vary among laser systems.
Studies have reported an increased risk of anterior capsular tears with laser cataract surgery, especially if there is movement of the eye during capsulotomy creation. Discontinuous laser treatment can weaken the anterior capsule.
A clear cornea and adequate pupillary dilation are required for laser cataract surgery. The procedure is inadvisable in eyes with corneal scars or a history of radial keratotomy owing to the risk of skip lesions.
PRECISION PULSE CAPSULOTOMY
Benefits. The Zepto IOL Positioning System (Centricity Vision) applies gentle suction to the anterior capsule with a nitinol ring and then delivers a 4-millisecond pulse of energy to create an automated, round capsulotomy. The device has a smaller footprint and is less expensive than a femtosecond laser system. The latest model can be integrated with the phaco machine and controlled with the surgeon footpedal. Patient docking on an additional machine is not required, increasing efficiency compared to a femtosecond laser. The Zepto may be used with patients who have media opacities, a history of radial keratotomy, or a white cataract.
A study that compared manual CCC and precision pulse capsulotomy in eyes with white cataracts reported shorter surgical times, no Argentinian flag signs, and less use of trypan blue dye with the Zepto device.4
Drawbacks. Unlike a femtosecond laser for cataract surgery, the Zepto does not offer astigmatism management. Toric IOLs must be aligned and low levels of astigmatism treated with another approach or device (eg, manual arcuate incisions, excimer laser enhancements). Also, nuclear disassembly cannot be performed with the Zepto.
Patients must be able to fixate well for the Zepto treatment to be centered on the visual axis. They must also hold still for the duration of treatment.
CONCLUSION
I perform manual CCCs, laser capsulotomies, and precision pulse capsulotomies. Most of my patients are candidates for and given the option of an automated capsulotomy, whether with a femtosecond laser or the Zepto system.
I generally prefer laser cataract surgery for patients who receive an advanced technology IOL such as multifocal or toric IOLs because astigmatism management is crucial to achieving optimal results.
I tend to use the Zepto if astigmatism will be treated later, such as with adjustments to a Light Adjustable Lens (RxSight), and for individuals with irregular astigmatism who receive an IC-8 Apthera IOL (Bausch + Lomb). I also favor the Zepto to a femtosecond laser for eyes with white or brunescent cataracts. A larger (5.4 mm) capsulotomy is created in these cases.
I perform a manual CCC in most of my cases. This is my preferred approach to eyes with weak zonules.
1. Sharma B, Abell RG, Arora T, Antony T, Vajpayee RB. Techniques of anterior capsulotomy in cataract surgery. Indian J Ophthalmol. 2019;67(4):450-460.
2. Qian DW, Guo HK, Jin SL, Zhang HY, Li YC. Femtosecond laser capsulotomy versus manual capsulotomy: a meta-analysis. Int J Ophthalmol. 2016;9(3):453-458.
3. Teuma EV, Gray G, Bedi R, Packer M. Femtosecond laser-assisted capsulotomy with capsular marks for toric IOL alignment: comparison of tensile strength with standard femtosecond laser capsulotomy. J Cataract Refract Surg. 2019;45(8):1177-1182.
4. Ifantides C, Sretavan D. Automated precision pulse capsulotomy vs manual capsulorhexis in white cataracts: reduction in procedural time and resource utilization. J Cataract Refract Surg. 2023;49(4):392-399.

