



Most cataract procedures are routine, but corneal opacity and/or irregularities may impair surgical visualization. These issues can be addressed either simultaneously with a triple procedure or in stages with corneal transplantation performed first and cataract surgery completed later.
Sometimes, the risks of corneal transplantation outweigh the benefits. For example, the patient may be at increased risk of graft rejection, infection, choroidal hemorrhage, or secondary or worsening glaucoma. Monocular patients with corneal opacification and worsening cataracts merit special consideration, particularly if they functioned well before the cataracts developed.
Alternative strategies to improve vision without requiring corneal transplantation are preferred when the opacity is incomplete or a patient is at high risk of keratoplasty. This article discusses considerations and surgical techniques to facilitate cataract surgery in eyes with irregular corneas.
CONSIDERATIONS
Biometry. IOL calculations on eyes with opacified or irregular corneas can be challenging for a variety of reasons:
- Optical biometry may not penetrate the corneal opacity;
- Ultrasound measurements may be inaccurate owing to poor fixation; and
- Accurate keratometry readings may be impossible.
Obtaining multiple biometry measurements can increase accuracy. If the patient is not monocular, measurements from the contralateral eye can provide guidance. Patient education is also essential. They must understand that glasses and/or contact lenses will be necessary after surgery to achieve optimal vision.
The corneal surface. Anterior segment surgeons recognize the importance of optimizing the ocular surface before cataract surgery. When corneal opacities or irregularities are present, it becomes necessary to look beyond dry eye management and consider smoothing the ocular surface to maximize the view for cataract surgery. A superficial keratectomy or removal of the corneal epithelium before cataract surgery may be beneficial if the surface is irregular, such as in eyes with Salzmann nodular degeneration, anterior basement membrane dystrophy, or an edematous/irregular epithelium. Figure 1 shows an improved view after epithelial removal. Care must be taken in eyes with significant limbal stem cell deficiency or a neurotrophic cornea because regenerating the epithelium may be difficult.

Figure 1. A patient presenting with bullous keratopathy demonstrating a distorted view during cataract surgery (A). Enhanced surgical view following the removal of the epithelium (B).
A contact lens technique may be attempted on patients whose corneal surface is highly irregular with or without significant opacity from an irregular scar (eg, from prior trauma).1 In retinal surgery, an OVD is often placed both under and over the contact lens. For cataract surgery, however, the OVD can be placed on the surface of the cornea, under the contact lens only, to improve the view (Figure 2). The caveat for phacoemulsification is that the wound should be located more posteriorly than usual (eg, a scleral tunnel instead of a clear corneal main incision) so that the contact lens does not induce distortions during surgery.

Figure 2. A view of the hazy ocular surface during cataract surgery (A). Application of an OVD to the surface of an opacified cornea (B). Placement of a bandage contact lens over the OVD-coated cornea, which improves visualization for cataract surgery (C).
SURGICAL TECHNIQUE
Patient positioning. Depending on the location of the opacity, the main incision may have to be shifted temporally or superiorly to maximize visualization and space in which to work.2
Anterior capsular dyes. Anterior capsule visualization is important for capsulorhexis creation. Awareness of the capsule’s borders is important for lenticular emulsification, cortical removal, and IOL implantation. Capsular dyes can improve visualization in an eye with a challenging cornea. Trypan blue can stiffen the capsule without increasing its fragility.3,4 Brilliant blue G requires a longer contact time, whereas indocyanine green and gentian violet must be premixed.5
I use trypan blue not only for hazy corneas but also for keratoconic, ectatic, post–radial keratotomy corneas. The dye enhances surgical details, which is helpful when the view is distorted.
Illumination. The red reflex can be maximized by changing microscope lighting parameters. Most ophthalmic microscopes offer two types of illumination: paraxial and coaxial lighting (Figure 3). The paraxial light is offset from the oculars by a few degrees to optimize depth of field and minimize the red reflex. The coaxial light source is directly in line with the oculars to maximize the reflection from the retina and, consequently, the red reflex.6 In an eye with an opacified cornea, the paraxial lighting can worsen scatter and diminish intraocular details. Increasing coaxial lighting and decreasing paraxial lighting can maximize the view and provide the best possible red reflex.
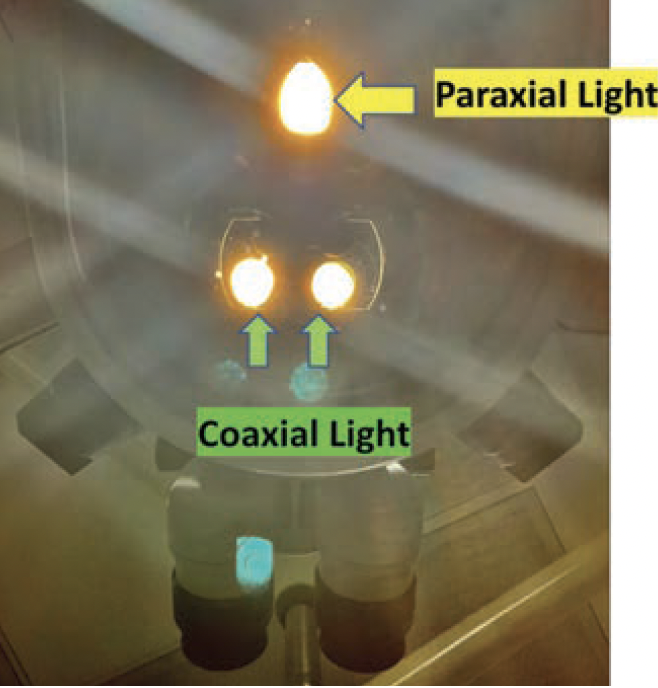
Figure 3. Illustration of paraxial and coaxial illumination in a surgical microscope. Paraxial lighting enhances the depth of field, and coaxial lighting is responsible for producing the red reflex.
Intracameral endoillumination. In 2003, Nishimura et al published an intracameral endoillumination technique in which an endoillumination probe is inserted into the anterior chamber via a limbal paracentesis site.7 In 2020, Tagle et al described passing a 23-gauge vitreoretinal light pipe through a paracentesis incision and into the anterior chamber to assist with cataract surgery.8 Smaller-gauge posterior segment vitrectomy light pipes have since become available and are less bulky for the anterior segment (Figure 4).
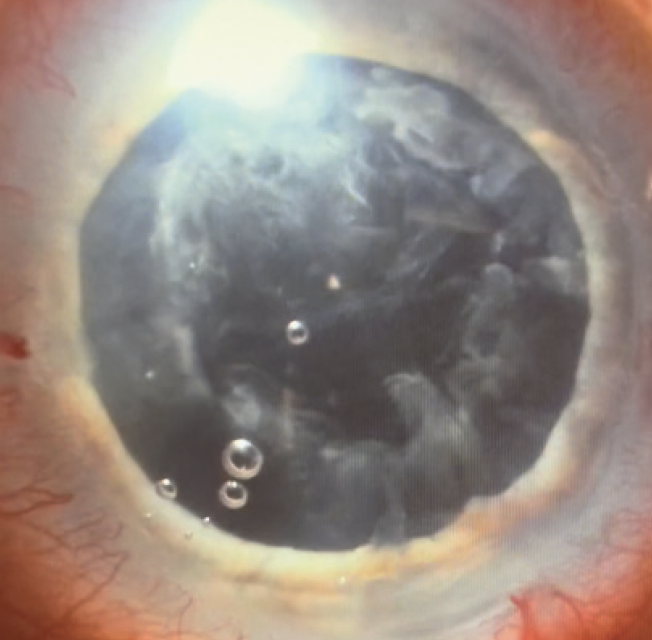
Figure 4. A 27-gauge retina xenon light pipe placed at the limbus illuminates details for cortical removal in an eye with an edematous cornea.
An alternative is the iChopper (Oculight), an FDA-approved intracameral endoilluminator with a chopping function for cataract surgery. The iChopper has a flat, noncutting tip with a light source at its end, making it ideal for horizontal chopping.9
Intravitreal endoillumination. As described by Oshima et al,10 intravitreal chandelier endoillumination involves a vitrectomy light pipe inserted transconjunctivally at the pars plana into the vitreous cavity, providing retroillumination to help visualize the cataract. This technique is helpful for anterior segment surgeons comfortable working in the pars plana space and those with assistance from a retina surgeon. It may not be practical for other cataract surgeons.
External illumination. Jacob et al described the application of external illumination obliquely at the limbus via a vitreoretinal endoilluminator light pipe to improve visualization of the orientation, fold, and position of an endothelial graft during Descemet membrane endothelial keratoplasty.11 This technique can also improve visualization during cataract surgery, but an assistant must hold the light source.
CONCLUSION
Not every eye with an opacified or irregular cornea requires a corneal transplant. In some instances, cataract surgery alone may be sufficient to improve the patient’s visual potential and quality of life.
Execution of the techniques described in this article requires adequate support and surgical expertise. Appropriate counseling is important to ensure that the goals of surgery align with patient expectations. The decision not to perform surgery is as important as the decision to proceed.
1. Tan JJ, George MS, Olmos de Koo LC. The bandage lens technique: a novel method to improve intraoperative visualization and fluidic stabilization during vitrectomy in cases of penetrating ocular trauma. Retina. 2016;36(7):1395-1398.
2. Sharma N, Singhal D, Maharana PK, et al. Phacoemulsification with coexisting corneal opacities. J Cataract Refract Surg. 2019;45(1):94-100.
3. Wollensak G, Spörl E, Pham DT. Biomechanics changes in the anterior lens capsule after trypan blue staining. J Cataract Refract Surg. 2004;30(7):1526-1530.
4. Coroneo MT, Pandey SK. Capsulorhexis integrity is unaffected by trypan blue: an in vitro study of human eyebank eyes. Investigative Ophthalmology & Visual Science. 2006;47(13):668.
5. Dada VK, Sharma N, Sudan R, Sethi H, Dada T, Pangtey MS. Anterior capsule staining for capsulorhexis in cases of white cataract: comparative clinical study. J Cataract Refract Surg. 2004;30(2):326-333.
6. Devgan U. Visualizing premium cataract surgery. Cataract & Refractive Surgery Today. November 2010. Accessed August 21, 2023. https://crstoday.com/articles/2010-nov/focus-on-surgical-micr-visualizing-premium-cataract-surgery
7. Nishimura A, Kobayashi A, Segawa Y, Sugiyama K. Endoillumination-assisted cataract surgery in a patient with cornea opacity. J Cataract Refract Surg. 2003;29(12):2277-2280.
8. Tagle AC, Armarnik S, Jiang K, Lyons CJ. Intracameral endoillumination-assisted cataract surgery in a child with opaque cornea. Can J Ophthalmol. 2020;55(4):e146-e148.
9. Kim H, Hwang SH, Eom Y, Nam DH. Improved visibility for illuminated chopper-assisted cataract surgery involving iris challenges. Indian J Opthalmol. 2023;71(3):757-762.
10. Oshima Y, Shima C, Maeda N, Tano Y. Chandelier retroillumination-assisted torsional oscillation for cataract surgery in patients with severe cornea opacity. J Cataract Refract Surg. 2007;33(12):2018-2022.
11. Jacob S, Agarwal A, Agarwal A, Narasimhan S, Kumar DA, Sivagnanam S. Endoilluminator-assisted transcorneal illumination for Descemet membrane endothelial keratoplasty: enhanced intraoperative visualization of the graft in corneal decompensation secondary to pseudophakic bullous keratopathy. J Cataract Refract Surg. 2014;40(8):1332-1336.

