



Have you ever remarked, “Today was a good day. Let’s do it again,” but found it impossible to replicate? It may be that all the puzzle pieces just happened to align perfectly on that day. For optimal clinic flow, four puzzle pieces must interlock seamlessly. I refer to these elements as the four S’s: space, staffing, systems, and scheduling. A close examination of each reveals the impact they have on one another.
Efficiency is defined as the capacity to achieve a goal with minimal wasted time and effort. The concept is applicable to at least two of the four puzzle pieces.
1. Space
Clinic flow is largely influenced by the office’s layout. Ideally, the clinic’s configuration minimizes the redundancy of steps for both patients and staff (Figure). The arrangement of equipment and rooms should align with the patient’s journey. For instance, if the initial workup is performed upon entry, the technicians’ lanes should be situated at the front of the clinic. Diagnostics might follow or be placed centrally for accessibility from any point. The final point of contact typically occurs in the exam room, which often leads to the optical area.
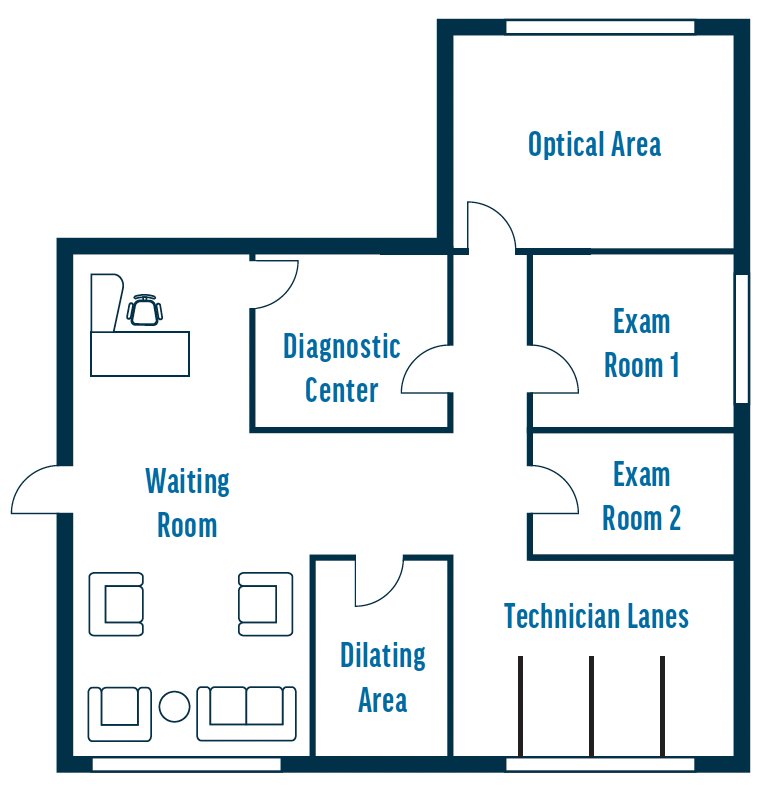
Figure. Example of an optimal clinic layout.
If your office lacks a central testing area, consider keeping tests that are frequently used together in the same space. An example would be positioning the biometer adjacent to the topographer, allowing the patient simply to turn their chair toward the second instrument. Eliminating their need to walk to another area for additional tests can shave seconds or even minutes off each workup.
2. Staffing
The COVID-19 pandemic affected the workforce significantly. Many workers did not return to their positions for various reasons, causing a staff shortage in medical practices. Hiring suitable candidates with or without experience has been challenging, and managers often wonder if new employees will show up for work or even stay. Innovative practices have begun cross-training their staff. The process can be implemented gradually, allowing one or two individuals at a time to become comfortable with their responsibilities. Potential job-sharing examples include the following:
- Call center with reception;
- Front desk staff performing eligibility and referrals, if handled by the business office;
- Technician and scribe; and
- Diagnostic technician and workup.
The current staffing shortage necessitates ongoing training for new hires and cross-training. A common concern is the lack of time for training now that patient volume has returned to prepandemic levels. An alternative is to train staff outside of working hours. Whatever the approach, observation is key. New hires should be paired with a patient and knowledgeable staff member who can explain the process and underlying rationale. If new employees do not understand the reason for a task, they may not become fully engaged. This is especially true of inexperienced technicians who may be eager to learn but lack experience. Even those with a medical background may feel that entering ophthalmology is like navigating a foreign country without knowing the language. To speak the language of eye care, they must learn it first. Various resources can help, including online platforms, books, videos, and on-site trainers.
During on-site training, removing new employees from the floor and providing the foundational knowledge they can then apply to the skills they acquire may help them become critical thinkers. If your practice uses an internal trainer, inform applicants that they are expected to work several evenings and/or Saturdays but will have time off during the week. This approach reduces overtime costs because only the trainer will earn overtime pay.
3. Systems
The term systems refers to the streamlining of processes rather than the software programs in place, although integration of the two is beneficial. Does your office provide patients with paper forms to complete and scan them despite implementing an electronic medical record system years ago? Many processes continue simply because a practice has always done it a certain way.
It may be time to evaluate and update manual tasks to electronic ones. For example, gather all demographic information during the initial call and print a sheet for patients to review at check-in rather than have them complete it for comparison. Combine multiple policies into a single form and use electronic signature pads for consent. These changes can reduce patient wait time. The medical history form has the greatest impact. Patients often take as long as 15 minutes to fill it out and frequently omit information. The technician must then enter the information into the electronic medical record. Instead, consider having technicians conduct interviews and bypass the form altogether.
Every technician should have a written copy of the doctors’ protocols based on the reason for the visit rather than the appointment type. This approach can minimize the number of questions directed to senior technicians and/or physicians.
4. Scheduling
The appointment template (see Appointment Scheduling Tips, pg 64) plays a significant role in clinic flow, but it is only one factor. The first principle of efficient scheduling is to avoid booking more patients than each physician can see in 1 hour. A time study may be required to determine the average duration of their time in the exam room. Stagger patient arrival times to prevent all providers’ patients from arriving simultaneously, which can cause a line to form at check-in unless there is sufficient staff to accommodate the number of patients booked. In the same vein, providers do not need to block their lunch hours at the same time. Spread out their and the staff’s breaks to permit patient appointments through the lunch hour.
APPOINTMENT SCHEDULING TIPS
- Stagger patient arrival times
- Avoid overbooking appointments
- Develop clear appointment types
- Limit the number of staff members authorized to overwrite the schedule
Develop appointment types and ensure all staff members understand the criteria for each one. Their clear comprehension of the schedule can reduce how often lengthy appointments are squeezed into shorter time slots. When multiple dilated exams are booked consecutively, physicians may find themselves with no patients to see before several must wait for their exams. Similarly, limit the number of staff members authorized to overwrite the schedule.
Applying the Four S’s to Your Practice
Each of the four S’s contributes to patient flow. To ensure a smooth start to the day, design a well-structured schedule, arrange for an appropriate number of staff members to assist patients upon arrival, and streamline processes. When each technician has a designated work-up room for patients, they do not need to spend time looking for an open one. By adhering to established protocols, unnecessary work-up components can be eliminated, expediting visits with the provider. This is particularly true when the initial, brief appointments are worked up in the doctor’s examination lane.
To identify bottlenecks in your office, walk through the practice as a patient or shadow a new patient scheduled for a comprehensive exam or consultation. During the process, ask yourself three questions:
- Am I retracing my steps?
- What redundancies do I observe?
- Is the staff actively engaged with patients or idle?
These observations may help you pinpoint areas in need of improvement. Exercise caution, however, and prioritize the most easily attainable solutions—the low-hanging fruit— before tackling more complex issues.

