



My experience with laser cataract surgery began in 2012. The goal of using a femtosecond laser is to improve the safety and reproducibility of the cataract procedure by reducing the number of surgical maneuvers performed. In my experience of approximately 9,500 procedures to date, a femtosecond laser offers advantages for complex cataract procedures.
MY TECHNIQUE
A major factor in the success of laser cataract surgery is the fragmentation pattern selected. When I began performing laser cataract surgery, common wisdom held that high energy resulted in better nuclear fragmentation. Experience has led me to the opposite conclusion: Low laser energy produces better fragmentation, fewer free radicals, less inflammation, and fewer bubbles. I have tried all the fragmentation patterns available—four, six, and eight segments; ice cubes; French fries; and the addition of one or two circular cuts. I currently favor six-segment division at 5.8 mm with two central circular cuts of 3 and 1.5 mm in diameter (Figure 1). I use a laser energy setting of 4.50 µJ (Figure 2). A small, central, round hole is created, and then the segments are separated with a nucleus manipulator spatula (Ligabue Manipulator, E. Janach). Separation is generally easy to perform without the need for ultrasound energy.
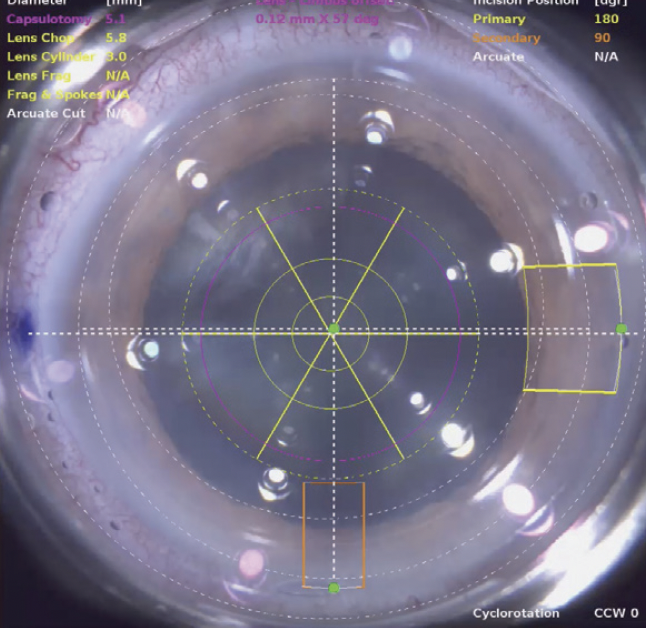
Figure 1. Fragmentation pattern using the LenSx Laser (Alcon).
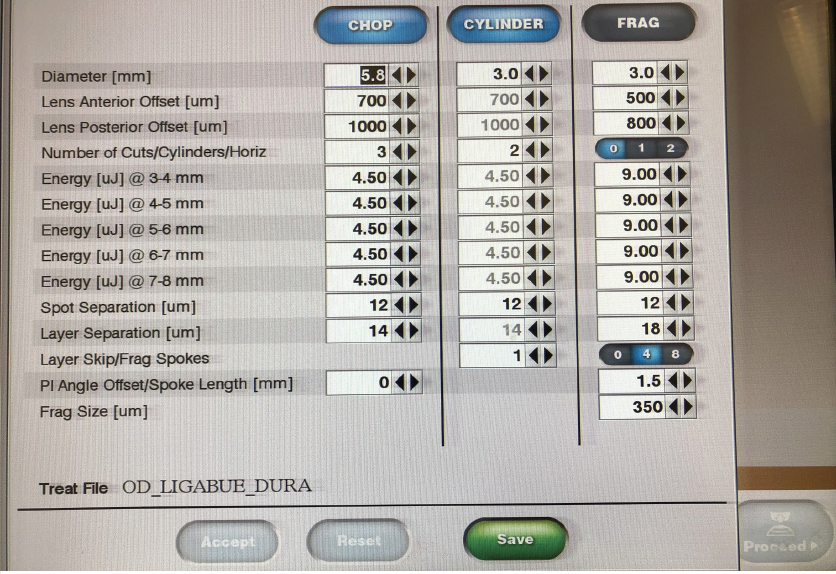
Figure 2. Energy settings.
My technique varies slightly for soft and medium to hard nuclei.
Soft nuclei. If the cataract is grade 1 or 2 (LOCS III classification), then a dedicated program on the Centurion Vision System (Alcon) with high vacuum (700+ mm Hg), an infusion pressure of 60 mm Hg, and no ultrasound energy is chosen to aspirate the fragments. The trick is to capture the pieces in the periphery because the material is softer.
Medium to hard nuclei. If the cataract is harder, infusion pressure is reduced to 20 or 26 mm Hg and the vacuum level is decreased to between 280 and 360 mm Hg. Low infusion pressure decreases turbulence in the anterior chamber and facilitates controlled manipulation of hard nuclear fragments. It is generally possible to work in the safe central zone of the anterior chamber, far from the endothelium and the posterior capsule.
CASE EXAMPLES
No. 1: Medium-hard nucleus. A femtosecond laser was used to divide the nucleus. The fragments were aspirated with vacuum but no ultrasound energy. (See the video below to watch the case.) The eye was quiet 1 day after surgery.
No. 2: Damaged posterior capsule. The posterior capsule of the eye in this case had been damaged during an earlier intravitreal injection of an antivascular endothelial growth factor. Laser fragmentation of the nucleus was performed. During aspiration, minimal rotation of the pieces and manipulation of the capsular bag were required, reducing the risk of extending the posterior capsular tear. (Scan the QR code to watch the case.)
CONCLUSION
The use of a femtosecond laser can decrease or eliminate the need for ultrasound energy during cataract surgery and reduce procedural time compared with standard phacoemulsification. A low energy setting can help safeguard the endothelium and decrease postoperative inflammation.

