
Premium IOLs raised the bar on refractive outcomes after cataract surgery. Toric implants can often free patients with high astigmatism from glasses or contact lenses for distance vision.1 In fact, in my experience, many such patients report seeing better than ever, because the astigmatic correction is closer to the nodal point, yielding a less distorted optical image.
The latest generation of toric lenses has been in clinical use for more than 8 years, but the precision and accuracy of their implantation could be improved. Femtosecond laser technology can help.
INCREASED PRECISION ENHANCES OUTCOMES
The traditional technique for implanting toric IOLs uses a nomogram that typically undercorrects the astigmatism slightly to avoid flipping the axis of corneal astigmatism. Measurements of corneal astigmatism often vary among different tests. For example, the power measurements determined by corneal topography and manual keratometry can differ, in which case the surgeon usually opts to use the lower-value toric lens power calculations. The lack of precision can leave the patient with residual corneal astigmatism.
To maximize refractive outcomes, I now employ laser cataract surgery for all patients undergoing cataract surgery with a toric IOL. I use the laser to create arcuate incisions (AIs) that are not opened at the time of surgery but rather postoperatively at the slit lamp to address any residual astigmatism. Based on optical coherence tomography imaging of the patient’s cornea, the laser creates incisions with precise depth and arc length that are difficult to match in traditional surgery using a diamond knife, pachymetry, and ink marks that are normally several degrees wide.
For all patients receiving a toric IOL, I create two AIs with at least 20º of arc and 85% depth at the 9-mm optical zone on the axis of astigmatism. Opening them later in the office corrects approximately 0.50 D of astigmatism. I find that this technique enhances the precision and accuracy of astigmatic management in three ways.
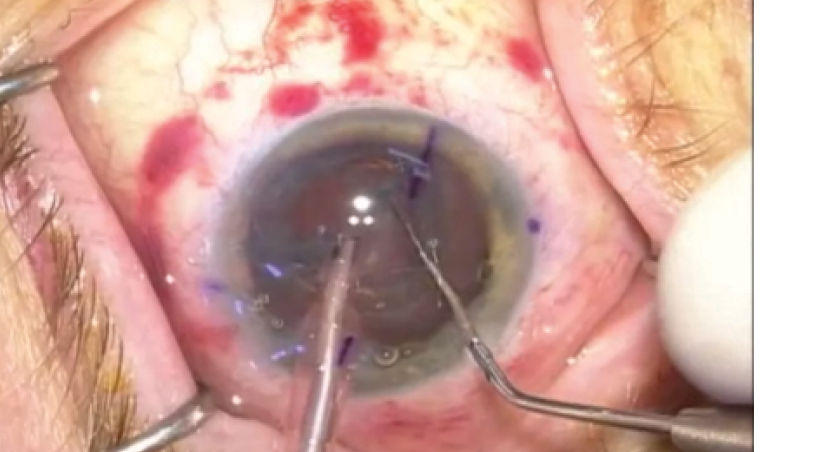
The author demonstrates how astigmatic keratotomy incisions created by the LenSx Laser (Alcon) can maximize outcomes with a toric lens. Click the image to watch the video.
First, if a patient has residual astigmatism after 2 weeks, I have the option of opening one or both AIs with a Sinskey hook at the slit lamp in the office. Postoperative management of the astigmatism allows me to address both nomogram undercorrection and variations in preoperative measurements of corneal astigmatism. For example, preoperative topography may show 2.00 D of astigmatism but manual keratometry only 1.50 D; 2 weeks after surgery, the corneal edema typically resolves, allowing any residual corneal astigmatism to be accurately measured and managed.
Second, I can use the imaging system of the laser platform to guide where I mark the axis for alignment of the toric IOL. I end up making two short marks on the cornea on the axis of astigmatism. I place ink marks at 90º and 270º while patients are sitting in the preoperative area. Then, during the laser procedure, the imaging system allows me to rotate the AIs to the axis based on the preoperative markings, thus adjusting for any ocular rotation when the patient is supine. This eliminates my need for axial markers and, in my estimation, increases precision.
Finally, the AIs serve as corneal “tattoos” on the axis of astigmatism, so months or years later, a dilated examination allows me to ensure that the toric IOL remains on axis. If a capsulotomy is performed later, the AIs will allow me to observe any rotation of the toric IOL at follow-up visits.
REDUCING RISKS
Traction
A toric lens is placed inside the capsular bag, so a tear in the capsule, zonular dehiscence, or vitreous loss would usually prohibit this IOL’s use. Minimizing traction on the capsular bag during surgery may reduce these aforementioned risks, especially in a patient with pseudoexfoliation or a history of trauma. Whereas traditional cataract surgery places stress on the capsule during the creation of a capsulorhexis, a femtosecond laser opens the capsule without traction on the bag
The laser procedure does not require rotation of the lens prior to its removal in my technique, again sparing the capsular bag. I viscodissect the anterior lens to the equator, while air bubbles from the laser treatment pneumodissect the posterior lens from the capsular bag, thus freeing adhesions and allowing the quadrants cut by the laser to be removed without rotating the lens. Additionally, I use the laser to cut four cylinders—the largest 4.7 mm in diameter—in the core of the lens along with a chopping pattern 5.3 mm in length. This approach allows me to “bowl” out the core of the lens and still crack the lens into quadrants with minimal manipulation inside the capsular bag compared with traditional sculpting and cracking.
Finally, optical coherence tomography imaging allows the laser to cut the lens within 500 µm of the posterior capsule. Knowing the lens’ thickness takes the guesswork out of how deep into the lens to phacoemulsify, and in my opinion, thereby decreasing the risk of a posterior capsular tear. Now, I can confidently remove the majority of the densest part of the cataract inside the capsular bag with reduced phaco power and minimal movement of the capsular bag.
Lens Position
During laser cataract surgery, I use interactive imaging to determine the size and placement of the capsulotomy. Using the computer’s mouse, I move the capsulotomy circle into position based on a live image of the patient’s eye. I create a 5-mm circular opening, which allows me to effectively center the IOL during surgery while leaving enough capsule to cover the implant by 0.5 mm evenly around the lens. This should result in a better lens position as the capsular bag contracts around the lens over time. IOL centration in relation to the capsular opening influences the centration of the lens and its position in the eye, in turn affecting the final refraction.2 A small capsular opening could displace the IOL posteriorly, leaving the patient hyperopic. A large opening could allow forward displacement of the IOL, inducing a myopic shift. An asymmetrical opening could torque the implant, creating astigmatism on the axis of rotation. I believe the precision of the laser capsulotomy allows for a more consistent refractive outcome based on the lens’ position.
CONCLUSION
The precision and accuracy of femtosecond laser technology can benefit patients undergoing cataract surgery in terms of safety and refractive outcomes with a toric IOL. Over time, imaging and preoperative data will improve, leading to new applications of the technology.n
1. Ale JB, Power J, Zohs K, Cunningham F. Refractive and visual outcome of toric intraocular lens implantation following cataract surgery. Nepal J Ophthalmol. 2012;4(7):37-44.
2. Filkorn T, Kovacs I, Takacs A, et al. Comparison of IOL power calculations and refractive outcome after laser refractive cataract surgery with a femtosecond laser versus conventional phacoemulsification. J Refract Surg. 2012;28:540-544.
Scott E. LaBorwit, MD
• president of Select Eye Care in Towson, Marylandv assistant professor, part-time faculty, at The Wilmer Eye Clinic, Johns Hopkins Hospital, Baltimore
• (410) 821-6400; sel104@me.com
• consultant to Alcon

