



Cataract surgery is the most commonly performed surgical procedure and one of the safest. Approximately 20 million cataract surgeries are performed worldwide every year. Intraoperative complications can occur sometimes and IOL implantation can be challenging in this setting.
Cataract surgery and IOL implantation in the presence of a torn posterior capsule and zonular dialysis can challenge novice and experienced surgeons. For eyes with inadequate zonular support or minimal residual sulcus, we have found it helpful to use a nylon suture as a leash to reduce the risk of a dropped IOL (Figure 1)—the IOL sling technique. This article and the accompanying video (watch below) describe the simple and effective method for primary or secondary IOL implantation in eyes with weak or absent zonules.
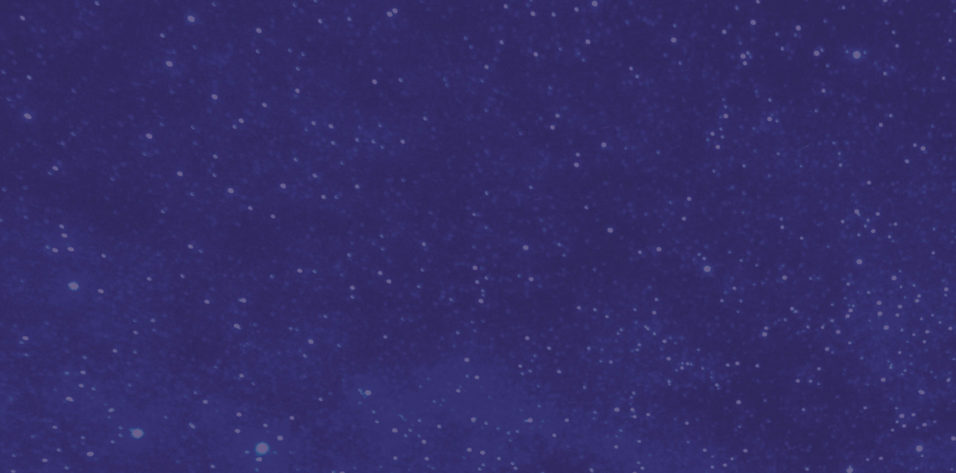
Figure 1. The IOL drops into the vitreous.
Figure 2. Before the IOL is implanted, a 9-0 or 10-0 nylon suture is introduced into the dialing hole of a three-piece rigid IOL (A and B).
Figure 3. Demonstration of the suture being passed through the dialing hole of the IOL (A and B).
Figure 4. The IOL sling is introduced through the sclerocorneal tunnel.
Figure 5. The leading haptic is placed in the sulcus.
Figure 6. The trailing haptic is placed in the sulcus.
Figure 7. The suture part of the IOL sling (blue arrows) remains outside the anterior chamber.
Figure 8. One arm of the sling is cut.
Figure 9. The suture is gently removed through the sclerocorneal tunnel.
Figure 10. The IOL sling technique is used during implantation of a retropupillary iris claw IOL.
FOUR EASY STEPS
No. 1. A 9-0 or 10-0 nylon suture is passed through the dialing hole of a three-piece rigid IOL (Figure 2 and Figure 3).
No. 2. The IOL with the 5- to 10-cm sling is introduced into a sclerocorneal tunnel that is approximately 7 mm in size (Figure 4).
No. 3. The leading haptic of the IOL is placed in the sulcus first (Figure 5), followed by the trailing haptic (Figure 6). During each step, the ends of the sling remain outside the anterior chamber (Figure 7).
No. 4. After the IOL has been positioned and is stable in the sulcus, one side of the suture is cut (Figure 8), and the suture is gently removed through the sclerocorneal tunnel (Figure 9).
ADDITIONAL APPLICATIONS
Externalization of the trailing haptic is often challenging during the scleral fixation of a sutureless IOL. The IOL sling technique can come in handy here because it prevents the haptic from slipping and causing the IOL to tilt.
During retropupillary iris claw lens implantation, the IOL sling technique can eliminate the risk that the IOL will drop into the vitreous during enclavation (Figure 10). This can be especially helpful for novice surgeons.
The IOL sling technique can also be useful in surgical settings with limited resources because it reduces the risk of complications, which can require more equipment.
CONCLUSION
The IOL sling is a simple and effective technique that adds another level of safety to IOL implantation.

