



I met H. Burkhard Dick, MD, PhD, in 2013 and asked him how I could improve the efficiency with which I removed a nucleus after prefragmentation with a femtosecond laser. He answered, “It is really a different procedure, isn’t it?”
Professor Dick’s response to my simplistic question profoundly influenced my approach. Paying close attention to the differences between nuclei that have and have not been presoftened has allowed me to adjust my surgical approach. This article shares a few techniques I use to crack a cataract that has been pretreated with a femtosecond laser. I have found that dividing the nucleus as soon as possible is the single most important step toward increasing efficiency.
ENDOLENTICULAR VISCODISSECTION
I developed a technique called endolenticular viscodissection as a method of cracking the lens. It also turns out to be a good way to estimate the effect of the femto-fragmentation and lens density. After the anterior chamber has been filled with an OVD, the tip of a 30-gauge cannula on a Healon syringe (Johnson & Johnson Vision) is pressed against the central capsule to confirm that the laser capsulotomy is free. One hand is used to inject an OVD into the central line of laser segmentation and advance the tip while the other hand secures the cannula hub. If the lens can be split in this way, a flash of Healon is often visible as posterior dissection occurs (Figure 1). Care must be taken not to overinflate the anterior chamber.
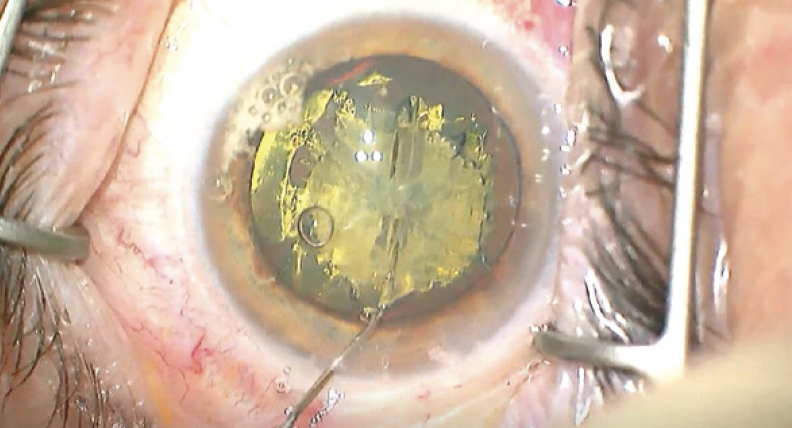
Figure 1. A flash of Healon can be seen during endolenticular dissection.
This test of nuclear density indicates how much phaco energy and time will be required to complete the fragmentation. If the nucleus does not split, then the cataract is solid enough centrally for the use of a quick chop technique. If this approach is attempted on a prefragmented lens that is too soft—especially if a peristaltic pump is being used—then it will not be possible to occlude the phaco tip with nuclear material.
COMPRESSION CHOP
What I call compression chop is performed if the lens is too hard for endolenticular viscodissection or quick chop—when the phaco tip cannot be buried in the central nucleus.
The technique begins with placement of the chopper in the nasal part of the segmentation line through a sideport incision. I favor the Scott femto chopper (Duckworth & Kent/Crestpoint) for this purpose. A Bechert nucleus rotator blunt fork is placed through the main incision, rotated to a vertical position, and aligned with the central segmentation line. Both instruments are simultaneously brought to the center, and the two opposing forces compress the central lens in the horizontal plane without placing stress on the zonules or capsule (Figure 2).
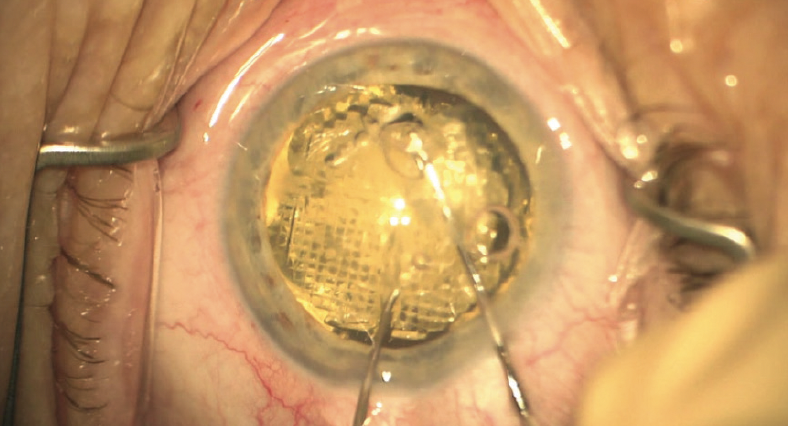
Figure 2. During compression chop, a chopper and Bechert nucleus rotator blunt fork are simultaneously brought to the center, and the two opposing forces compress the central lens in the horizontal plane.
With a black cataract, it may not be possible to enter the segmentation line, and care must be taken not to exert too much force posteriorly. If necessary, a miLoop (Carl Zeiss Meditec) may be used to divide the nucleus.

