


CASE PRESENTATION
A 58-year-old woman is referred to you for a cataract surgery consultation. The patient has a moderately dense cataract and 2.00 D of regular astigmatism. She shares that her friend had cataract surgery performed by another doctor in your community. Not only can he see without glasses after surgery, she says, but he didn’t have to pay anything extra for it. She’s adamant that you do her surgery just like her friend’s.
QUESTIONS FOR THE PANEL
1. How do you approach patients who desire spectacle independence and refuse to pay extra for astigmatism-correcting and/or presbyopia-correcting IOL technology?
2. What patients hear from their friends is not always accurate. How do you navigate through the noise from friends, family, and the internet when counseling patients regarding their options for spectacle independence with cataract surgery?
3. What would your explanation be for why the patient would benefit from a toric IOL even though her friend didn’t have to pay anything?
4. Are there any options for the patient that avoid all out-of-pocket costs?

Allon Barsam, MD, MA, FRCOphth
The patient must be advised that most presbyopia-correcting and presbyopia-correcting toric IOLs require an out-of-pocket cost. The expense to the patient covers the additional cost of the IOL, the skill and diagnostic technologies required to choose and implant an advanced technology IOL safely, and any additional care required after cataract surgery such as a laser enhancement.
I would explain to the patient that paying for an advanced technology IOL is likely to save her a significant amount of money over the next few years compared to what she would spend on spectacles in the same timeframe. I would also explain that the IOL is selected and the power customized to meet her visual needs and work best with her individual optical system. Lastly, I would spend time educating the patient that no single lens works in everyone’s eye. In other words, what worked for her friend might not work for her. The patient has astigmatism that might not have been present in her friend’s eyes. The patient should be advised that eyes with astigmatism require a different and more expensive lens than her friend received to maximize the chance of spectacle independence.
With respect to presbyopia, I would explain that a small percentage of patients are lucky enough to be able to read without glasses despite having a standard (ie, monofocal) lens but that they are the exception rather than the rule.
Monovision may be an option to address the patient’s presbyopia, but it will not address her astigmatism. The astigmatism can be corrected with a toric IOL or a surgical approach such as limbal relaxing incisions. An incisional approach, however, is not as accurate or as safe as a toric IOL, especially in the presence of higher amounts of astigmatism such as the patient has.


Arjan Hura, MD, and Neda Shamie, MD
Part of the art of refractive cataract surgery is delivering or surpassing the patient’s expected postoperative outcome. The groundwork for success is laid before surgery. Patient expectations are often influenced by what they read online, the experiences of their friends and family members, and direct-to-consumer marketing by IOL manufacturers. It is the surgeon’s job to assess each patient’s understanding of cataract surgery and the various options for vision correction in addition to addressing any misconceptions and refining expectations to be appropriate. This can be a time-consuming task, but it is crucial to set realistic expectations before surgery.
We would emphasize to the patient that her refraction and ocular anatomy are unique and likely differ from those of her friend. We would note, for example, that her friend might not have had astigmatism, might have a small amount of astigmatism that does not affect his postoperative satisfaction, or might have residual with-the-rule astigmatism that is contributing to functional depth of focus.
We would carefully explain the concept of astigmatism and the patient’s particular situation to her. We would emphasize that, if her astigmatism is not corrected, she will likely need to wear spectacles after surgery. Given her amount of astigmatism, a toric model of either an extended depth of focus (EDOF) or trifocal IOL is the best option for astigmatic correction. If the 2.00 D of astigmatism is corneal, with the rule, and in the nondominant eye, we would also discuss the option of monovision because the spherical equivalent might confer acceptable myopic defocus. If the patient desires spectacle independence but without the additional cost of a toric IOL, a less expensive (and likely less predictable) alternative for astigmatism correction is the placement of limbal relaxing incisions at the time of surgery.
Ultimately, it is the surgeon’s responsibility to educate patients, set appropriate expectations, explain the options available for vision correction, and provide the best possible visual outcome for the patient’s unique situation.

Guy Sallet, MD, FEBOphth
If cataract surgery on the patient’s friend involved no extra costs, he probably received monofocal IOLs. It is unknown whether the friend had preoperative astigmatism. I would address the patient’s questions scientifically first and then elaborate on the different options and their financial implications.
ASTIGMATISM CORRECTION
I would educate the patient on the concept of astigmatism and explain that the amount of astigmatism that she has makes it likely that she will need spectacles after surgery if she receives a standard monofocal IOL. I would add that the implantation of a toric IOL would increase her chance of achieving good UCVA and greater spectacle independence after surgery. I would cite a systematic review in which 70% of patients who received a toric IOL and 46.8% of patients who received a nontoric IOL never wore spectacles for distance vision postoperatively.1 The review included studies with patients who had 0.75 to 3.00 D of astigmatism. In the case presented here, the patient has 2.00 D of astigmatism, which means that she will probably need spectacles after surgery.
I would then tell the patient that toric IOLs are more expensive than standard monofocal IOLs but that toric IOLs should be an economical option in the long run. I would cite economic analyses showing that the lifetime costs of patients with preoperative corneal astigmatism are lower if they receive a toric IOL because of their reduced need for spectacles and/or contact lenses after surgery.2 I would add that accurately calculating the degree and axis of astigmatism requires precise biometry and, potentially, supplementary topography and/or tomography and that the cost of these diagnostics are included in the fee for a toric IOL.
FREEDOM FROM GLASSES
I would tell the patient that there is a good chance of achieving spectacle independence for distance vision with modern cataract surgery and a standard monofocal IOL. I would then state that a variety of surgical strategies are available for increasing people’s freedom from glasses for distance, intermediate, and near vision for an extra cost.
A monovision strategy, for example, that targets the dominant eye for distance and the nondominant eye for near is a low-cost option. In a study that compared outcomes with monofocal, EDOF, and trifocal IOLs, 92% and 70% of patients who received trifocal IOLs and monovision with monofocal IOLs, respectively, achieved spectacle independence.3 I would tell the patient that, based on these data, her friend is lucky not to need spectacles after cataract surgery with a monofocal IOL.
I would then tell the patient that my practice offers advanced IOL technology to maximize patients’ chances of achieving spectacle freedom and that the greater value comes at an extra cost. I would explain that EDOF IOLs generally provide better intermediate vision than monofocal IOLs but that patients typically need to wear reading glasses. I would then state that trifocal IOLs are designed to decrease spectacle dependence at distance, intermediate, and near. I would note that trifocal IOLs cost more than EDOF IOLs, which in turn cost more than standard monofocal IOLs. If this patient wants complete spectacle freedom, toric trifocal IOLs are not the cheapest option, but they are the best chance to achieve her goal.
1. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123(2):275-286.
2. Laurendeau C, Lafuma A, Berdeaux G. Modelling lifetime cost consequences of toric compared with standard IOLs in cataract surgery of astigmatic patients in four European countries. J Med Econ. 2009;12:230-237.
3. Rodov L, Reitblat O, Levy A, Assia EI, Kleinmann G. Visual outcomes and patient satisfaction for trifocal, extended depth of focus and monofocal intraocular lenses. J Refract Surg. 2019;35(7):434-440.

Stefanie Schmickler, MD
The preoperative consultation is a major factor in how successful the patient feels cataract surgery is.
APPLES AND ORANGES
In situations like this one, my first step is to tell patients, “You cannot compare apples with oranges. Your eyes are unique and require individualized treatment.”
I would describe the patient’s refractive error and explain that she has regular astigmatism. I would show her the bowtie pattern on corneal topography and compare it to normal topography (Figure 1). I would add that her friend’s ability to see without glasses suggests that he did not have astigmatism and would note that premium surgical options are required if she desires spectacle independence.
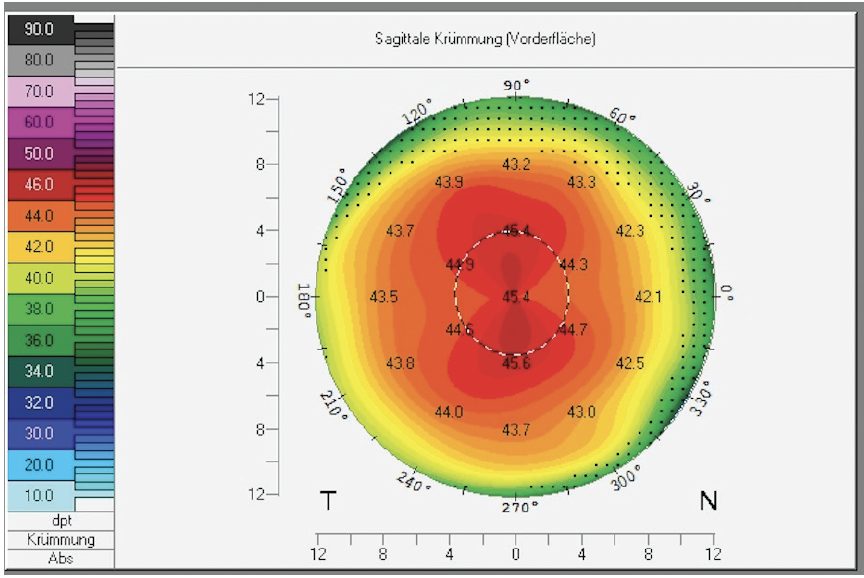
Figure 1. A bowtie pattern on topography showing regular astigmatism.
Next, I would inform the patient that correcting astigmatism with a lens requires more complex surgical planning and a toric IOL, which costs more than a standard monofocal IOL. On the day of surgery, the axis of astigmatism must be marked. I would emphasize that the additional work and costs involved are not covered by standard reimbursement.
PRESBYOPIA CORRECTION
If the patient wishes to receive a presbyopia-correcting IOL, I would note that candidacy for the technology requires a healthy cornea and an absence of glaucoma and retinal disease. Additionally, the eye must have a low level (< 0.3 µm) of higher-order aberrations (Figure 2), and I would perform the measurement at that time. Next, I would show a picture demonstrating halos (Figure 3) and explain that the patient might have to tolerate this visual phenomenon after surgery. About two-thirds of my patients no longer want a multifocal IOL after seeing the picture. The other one-third say that they already see halos at night and are not disturbed by the prospect.
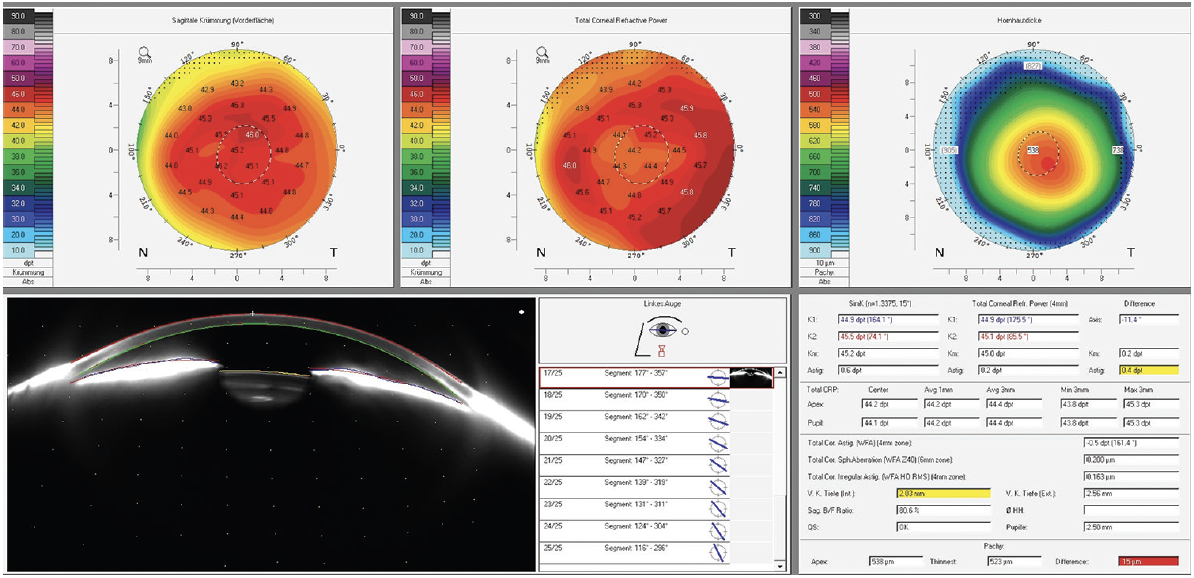
Figure 2. An eye with a low level (< 0.3 µm) of higher-order aberrations and total corneal irregular astigmatism.

Figure 3. Images depicting the effects of halos and glare.
Figures 1–3 courtesy of Stefanie Schmickler, MD
If the patient elects presbyopia correction, I would emphasize that a plano result cannot be guaranteed. I would state that a residual refractive error could make spectacle correction necessary after surgery. If a refractive enhancement with a laser is required, then there will be an extra cost for which the patient is responsible. I find that only patients who sign an agreement to this effect preoperatively are satisfied with their postoperative results.
MONOVISION
Unless corrected, 2.00 D of regular astigmatism will compromise the patient’s visual acuity after surgery. Even a refractive target of -2.00 D for reading without glasses will not satisfy her because her reading vision will not be clear. Furthermore, in my experience, unless patients have a history of successful monovision, they rarely adapt to it. An additional point is that patients with monovision are required to wear spectacles when driving in Germany, where I practice.
CONCLUSION
When talking with patients, I compare standard and premium cataract surgery to driving to Rome in a Fiat 500 and a Mercedes-Benz S-Class, respectively. Either car will get them there, but they will certainly be more comfortable in the Mercedes, although at a higher cost.

Karl G. Stonecipher, MD
We’ve all seen our share of patients who insist that they receive the same care and results as their friends—and at the same cost. We’ve also all had patients come back after their surgery saying, “You promised me XYZ.” Both scenarios do only two things: (1) They make your staff miserable, and (2) they take up chair time in your clinic.
TACTICS FOR MORE EFFICIENT COUNSELING
A picture is worth a thousand words. I love the Optical Quality Analysis System software created by Damien Gatinel, MD, PhD, and available on the OPD Scan III (Nidek). The images it produces show patients what they can expect with a monofocal IOL versus a toric IOL and help them visualize the distortions and blur that are caused by their astigmatism (Figure 4). Sharing these images during the preoperative evaluation facilitates a meaningful conversation between the doctor and patient. After showing these images, I find it to be easier to discuss the cost of the lens and its benefits in a way that patients can understand.
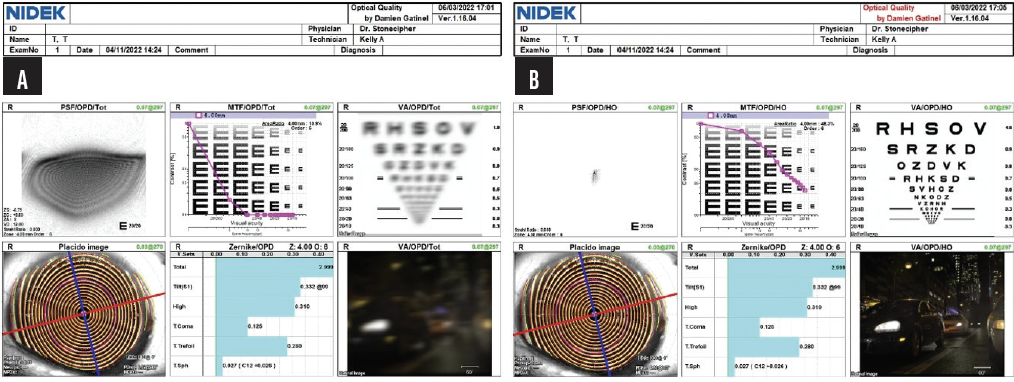
Figure 4. The preoperative testing demonstrates how astigmatism can affect the point spread function, modulation transfer function, visual acuity, and nighttime vision (A). The results of testing improve if a toric IOL is implanted (B).
Friends say one thing, but patients hear another. I tell patients that we are all unique and comparing the outcomes that different patients achieve is like comparing apples with oranges. Maintaining transparency about patients’ financial responsibilities helps them establish realistic expectations for their specific outcomes. All patients review a form that breaks down the costs of cataract surgery, including fees for the surgeon and surgery center; devices such as the IOL and femtosecond laser; and pre- and intraoperative analysis, including biometry, OCT, and topography. Patients sign the form and are encouraged to ask questions.
When talking to patients about their expected results, I use examples that they can relate to depending on their personal habits and hobbies. They are counseled that the technology they choose will affect their distance (eg, driving), intermediate (eg, cell phone, computer, cooking), and near (eg, reading small print on a prescription bottle or threading a needle) vision. I also find it helpful to use their personal data to demonstrate the difference between corneal and lenticular astigmatism. I show them similar images to personalize the benefits that can be achieved with a toric IOL (Figure 5) and demonstrate the differences in vision achieved with a spherical or monofocal IOL versus a toric IOL.
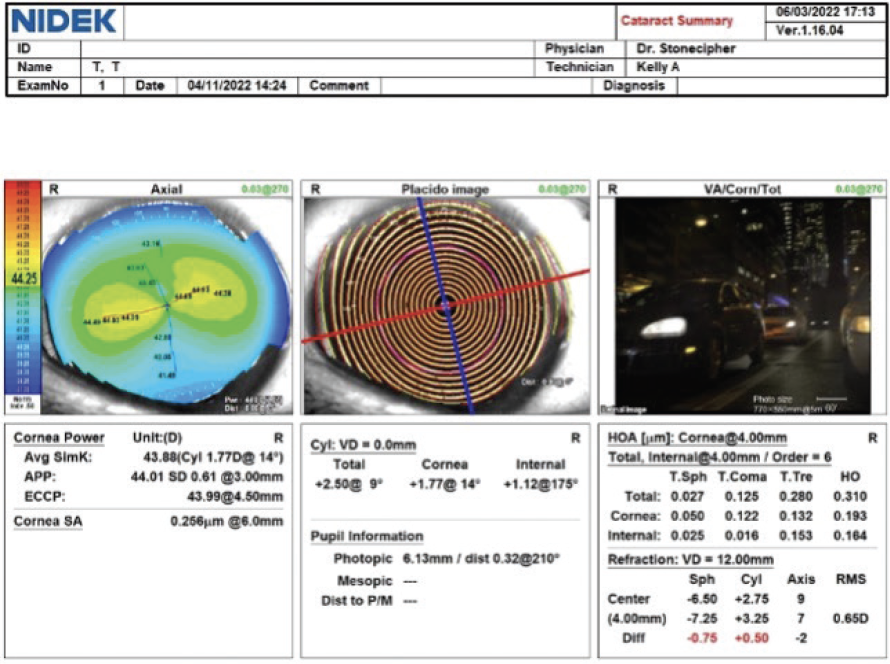
Figure 5. Information from the diagnostic testing can be used to explain to the patient the difference between lenticular and corneal astigmatism.
Figures 4 and 5 courtesy of Karl G. Stonecipher, MD
Let them drive the car before they buy it. My practice has more than 500 comanaging physicians, but only a few patients come in after having had a contact lens trial when appropriate. Patients pay out of pocket for a contact lens trial, and I tell them that it is the only way they can know what to expect after surgery. I explain that their cataract may limit the overall benefits of a contact lens trial but that they should get a general picture of what they can expect to achieve. A contact lens trial can also help them experience scenarios such as monovision and eliminate surprises. Sometimes, hearing the same comments from a different physician is helpful and prevents the patient from later saying, “You never told me I wasn’t going to read with this special lens.”
Talk about what patients can get without paying extra. Most patients with a significant level of astigmatism are used to buying contact lenses or glasses. I like to discuss the cost of these expenditures. The continued expense of contact lenses and glasses can easily be higher than the average cost of a toric IOL implanted with or without the use of a femtosecond laser for cataract surgery and intraoperative diagnostics.
Don’t promise patients that they will achieve spectacle independence. I explain that an additional intervention such as laser enhancement, IOL rotation, or IOL exchange may be required after surgery to achieve their target refraction. Patients typically do not like hearing this, but total transparency can prevent their future dissatisfaction. I bear in mind something that Eric D. Donnenfeld, MD, once said: “It’s not your problem until you do their surgery. Then, it’s yours forever.”

Blake K. Williamson, MD, MPH, MS
This is a common situation. First, I would tell the patient that insurance providers tend to cover only what they consider to be the medically necessary parts of a procedure. Toric IOLs aren’t covered because patients can wear glasses or contact lenses after surgery. In other words, I would say, “Toric IOLs are not medically necessary, but they can greatly improve your quality of life. Insurers therefore view toric IOLs and LASIK, for example, to be a cosmetic or lifestyle benefit.” Most patients understand this explanation. If they refuse to pay for astigmatism- or presbyopia-correcting IOLs, then they are not great candidates for the technology, and I do not offer it to them.
Next, I would tell the patient that hearing about friends’ and neighbors’ cataract procedures can be confusing because their eyes and situations are different from the patient’s. I would emphasize that no two eyes are exactly alike. I would explain that her friend probably had minimal corneal astigmatism and was therefore able to attain what I call GEV, or good enough vision, meaning that the friend can function without glasses. That’s good news for the friend but irrelevant to the patient, who has a lot of corneal astigmatism.
I would then explain the concept of astigmatism and show the patient her astigmatism on topography. Seeing is believing for many people. I would tell her that low- and no-cost options for presbyopia correction are available but that they are not suited to her because of her astigmatism.

Shannon Wong, MD
I would begin by explaining to the patient that every eye is unique. I would state clearly that I cannot comment on patients I do not know and have not examined. What I can comment on is the patient in the room with me because I can evaluate the condition of her eyes.
I would then tell the patient that paying the minimum for cataract surgery means receiving a standard monofocal IOL. I would inform her that she has preexisting astigmatism but that she is not required to pay for a more expensive IOL or surgical intervention to correct it. I would explain that, with a standard monofocal IOL, she can expect to wear glasses all or most of the time after surgery to have clear vision.

