



This story began in 2013, when a 57-year-old man entered my office asking for refractive surgery. His eyes were slightly hyperopic, with manifest refraction of about +1.75 D (Table). He was wearing spectacles only for near, but he stated that he was suffering with distance vision impairment.
Because of his age, because he had a job that was not visually demanding, and because his cornea was regular (Figure 1A) and his lens transparent, I suggested presbyopic LASIK (presby-LASIK) using the Supracor technique with the Teneo excimer laser (Bausch + Lomb), a procedure I began performing in 2011. The patient immediately accepted and signed the relevant informed consent form.
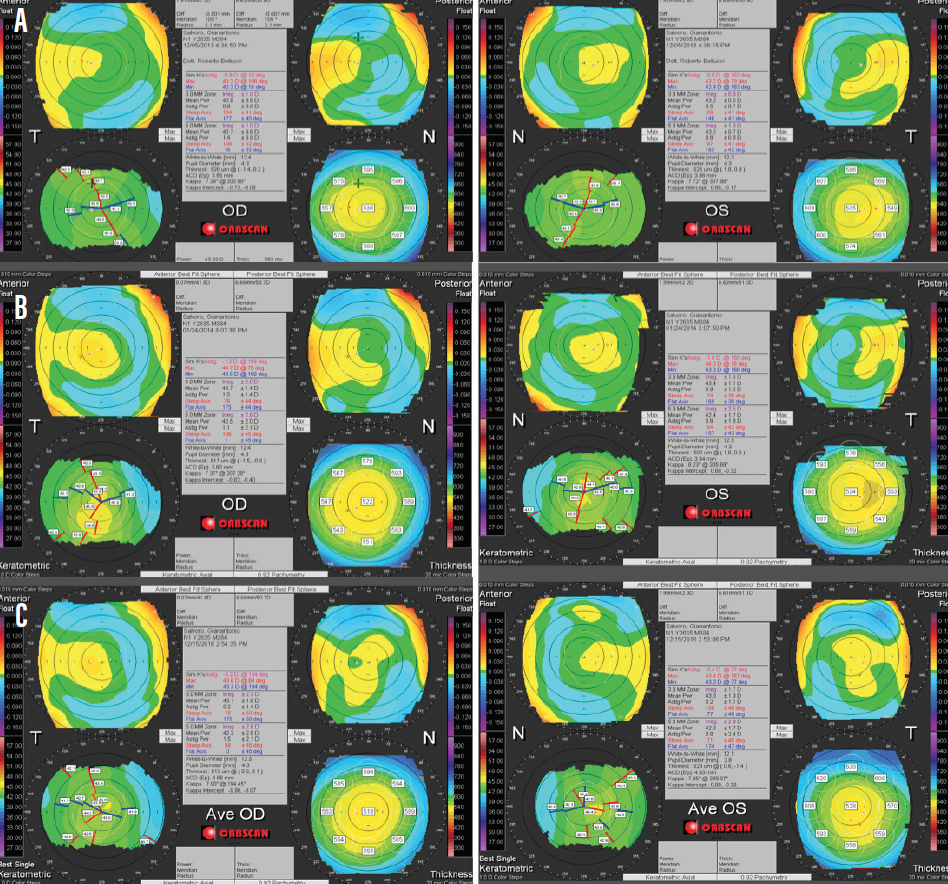
Figure 1. Corneal topography before surgery (A), after Supracor presby-LASIK (B), and after presby-LASIK retreatment to improve distance vision (C).
Surgery took place in June 2013 and was uneventful. The regular protocol, providing more spherical aberration to improve near vision, was used for the left eye; the mild protocol, providing less spherical aberration to favor distance vision, was used for the nondominant right eye.
The patient immediately acknowledged an improvement in near vision, but he complained about his distance vision, which in his opinion was poor and not good enough to allow him to drive. A waiting period did not help, and 6 months later he was still complaining. At that time, his binocular uncorrected near visual acuity (UNVA) was 0.1 logMAR and binocular uncorrected distance visual acuity (UDVA) was 0.02 logMAR. The manifest refraction is listed in the Table, and the corneal topography is shown in Figure 1B.
SECOND TRY
Because the patient was aggressive in asking for a solution, a retreatment with LASIK was scheduled. This treatment took place in September 2015, aiming for correction of the low myopic astigmatism in both eyes.
After retreatment, the patient’s corneal topography was acceptable (Figure 1C), and his UDVA was good. However, the patient now complained that his UNVA—despite a seemingly acceptable level of 0.2 logMAR, which was leaving him spectacle independent for 90% of his daily activities—was not acceptable.
The patient started presenting every week for an unscheduled visit, not forgetting to share his dissatisfaction with the other patients in the waiting room but always forgetting to pay for the extra visits. I wondered what was the cause of this dissatisfaction? What solution could I apply?
BACK FOR ANOTHER TREATMENT
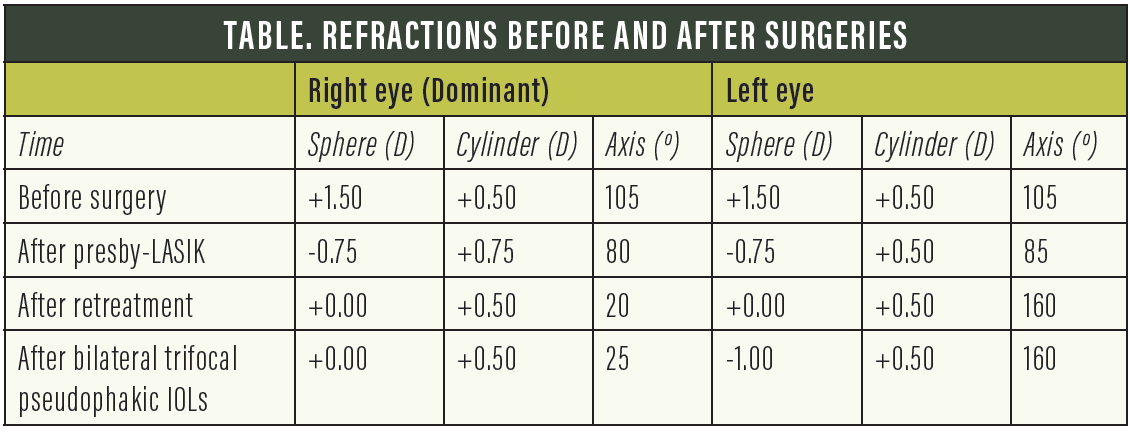
Because of his desire to look young, as indicated by his behavior, I decided to suggest refractive lens exchange as the ultimate way to achieve spectacle independence. I noted that his keratometry readings were now not so different from his original status (Figure 2) and that the aberration profile of both eyes was acceptable for multifocal IOL implantation (Figure 1C). I used the Aladdin biometer (Topcon) and the Barrett Universal II formula for IOL power calculation, with no special adjustment after the previous surgery.
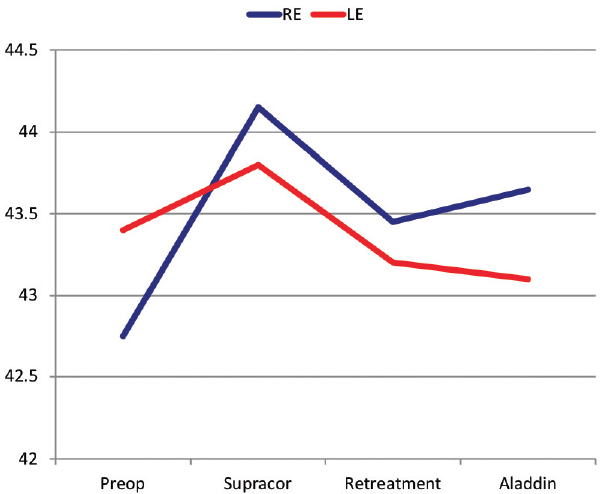
Figure 2. Simulated keratometry readings before and after the three surgeries. (Abbreviations: RE, right eye; LE, left eye)
Femtosecond laser–assisted refractive lens exchange was performed in December 2016 in the patient’s left eye and in January 2017 in his right. A 20.00 D FineVision Pod F trifocal spherical IOL (PhysIOL) was implanted in each eye.
Et voilà: Success! The outcome was minimal astigmatism in both eyes and a -0.50 D myopic outcome in his left nondominant eye. The aberration profile, measured with the Zywawe aberrometer (Bausch + Lomb), was good (Figure 3). The patient showed his satisfaction, mentioned how good his social life without spectacles was—he was not married—and disappeared for 2 months.
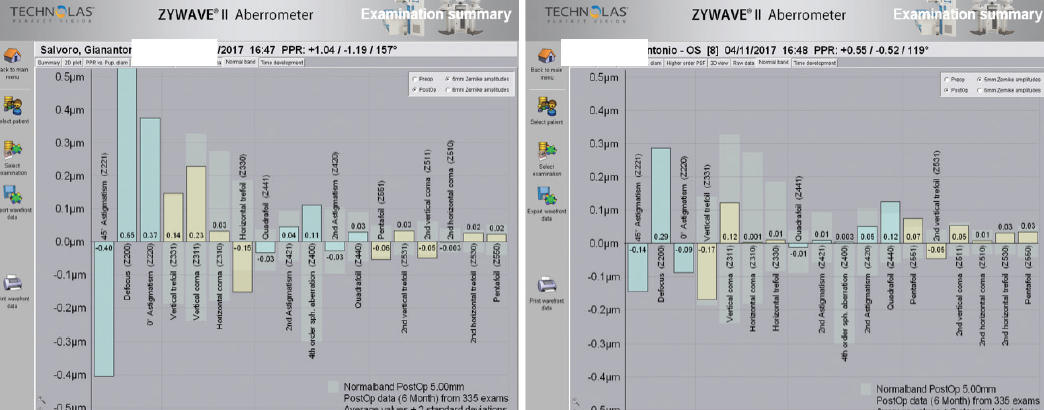
Figure 3. Aberration profile of the two eyes at the last follow-up visit.
BUT WAIT
But I had not been completely lucky after all. Two months later, he came back reporting intermittent blurry vision, something he had not experienced before. By this time, I was prepared: I verified his dry eye condition and suggested lubricants that worked fine for him. Still, the patient returned every month for 1 additional year, seeking a definitive solution of the dry eye problem, “even at the cost of new surgery.” I suggested a holiday in a humid place instead: “My prescription is 2 weeks in Bali.”
In late 2018, he finally disappeared from my office. Surely this was a difficult patient! However, even the most difficult patient can teach us something. I learned that, in my hands, trifocal IOLs are better than Supracor for older patients. And I still wonder whether it was dry eye, and not insufficiency of the Supracor procedure, that caused his original dissatisfaction after LASIK. No doubt, easy patients teach us less.

