




Despite many technical advances, visual axis obscuration (VAO) remains one of the major roadblocks that hampers visual rehabilitation after pediatric cataract surgery. The younger the child is, the more severe is the VAO.1-3 Further, early onset of VAO at a young age induces amblyopia4-7 and necessitates additional surgical procedures under general anesthesia.
Therefore, constant efforts are made by pediatric cataract surgeons to either reduce or delay the onset of VAO. Posterior capsulotomy with anterior vitrectomy has become a part of the routine surgical strategy for pediatric cataract management for the same reason in infants and children younger than 5 or 6 years.8,9
Neuhann and Neuhann first depicted optic capture of an IOL in an adult with posterior capsular rupture in a film presented at the 1991 ASCRS Annual Meeting. Subsequently, Gimbel and Debroff described this technique for pediatric cataract surgery and also advocated the technique as a means to altogether avoid anterior vitrectomy.10,11
Subsequently, conflicting results regarding the effectiveness of optic capture of rigid PMMA IOLs have been reported.12-15 However, with the introduction of innovations in foldable IOL materials and design, there has been renewed interest in the technique of optic capture in both adults and children.16-18
A SKILL-DEPENDENT PROCEDURE
Posterior optic capture of an IOL involves placing the IOL inside the capsular bag and then sliding the IOL optic through the margins of a posterior capsulorhexis (Figure 1). The advantages of this technique are dual:
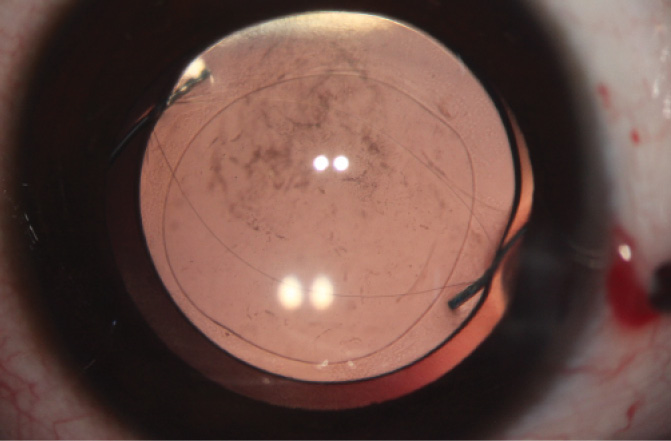
Figure 1. IOL captured through a posterior capsulorhexis, as indicated by ovalization of the capsulorhexis margin.
- First, it sequesters the lens epithelial cells (LECs) in the equatorial region of the capsular bag due to fusion of the anterior and posterior capsulorhexis margins. This prevents the LECs from migrating to the central visual axis, thereby preventing VAO or delaying significant encroachment of VAO into the central visual axis; and
- Second, it locks the IOL in position, preventing anteroposterior or lateral movement. This ensures stable IOL fixation in the desired position in the capsular bag.
Posterior IOL optic capture is definitely a skill-dependent procedure; however, with sufficient experience in performing posterior capsulorhexis, the creation of symmetrical, well-centered capsulorhexes can be mastered. Further, with the evolution of the use of a femtosecond laser in cataract surgery, applying this technology can allow surgeons to create precisely sized and centered anterior and posterior capsulorhexes. The margins of these posterior capsulorhexes are strong enough to allow posterior optic capture.
Anterior vitrectomy has undergone dramatic improvements with the introduction of high cut-rate vitrectors and 23- and 25-gauge sutureless trocar-cannula systems. However, vitrectomy is an additional procedure in cataract surgery, and there are no good data available on its impact on pediatric eyes, including its effect on axial growth of the eye. There is some speculation that anterior vitrectomy may be associated with a higher risk of developing open-angle glaucoma in aphakic or pseudophakic eyes.19 Therefore, any technique that can help to achieve the objective of reducing VAO and yet avoid this additional surgical maneuver would be helpful to surgeons.
Other techniques can also be employed to prevent or reduce VAO in young children without the need to perform an anterior vitrectomy, including the bag-in-the-lens technique and vertical entrapment of the IOL.20,21 Both of these techniques are also based on the principle of sequestering the LECs within the fused anterior and posterior capsular leaflets.
COMPARATIVE TRIAL
We recently published results of a randomized clinical trial comparing primary optic capture of a three-piece hydrophobic acrylic IOL without anterior vitrectomy versus primary in-the-bag IOL implantation of a three-piece hydrophobic acrylic IOL along with anterior vitrectomy in children up to 4 years of age (Figure 2).22
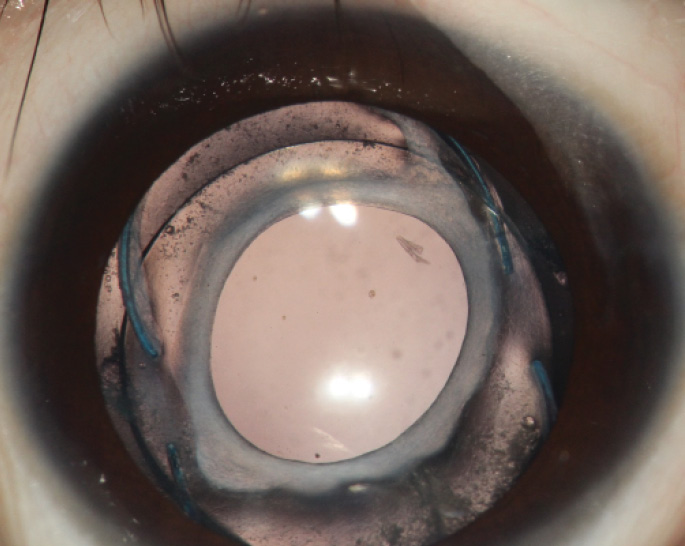
Figure 2. A pediatric patient at 12 months after surgery, showing optic capture of a three-piece AcrySof IOL (Alcon).
The results of this study showed that the incidence of VAO was comparable between the two groups. With up to 12 months of followup, there was no VAO in the optic capture group, compared with one eye needing a membranectomy in the in-the-bag-IOL group. It is important to note that there was no incidence of glaucoma, undue inflammation, or intraoperative adverse events in the optic-capture group.
TRAUMATIC CATARACTS
Another application of this technique that we find useful is in traumatic cataracts, particularly those in which the anterior capsule is discontinuous. In these eyes, even if an IOL is placed in the capsular bag, it may tilt or partially come out of the capsular bag and into the ciliary sulcus. In such cases, creating a posterior capsulorhexis and performing posterior optic capture ensures stable IOL positioning. As an additional advantage, there is reduction or retardation of VAO in these traumatic cataracts, which are often seen in younger individuals.
CONCLUSION
The technique of optic capture is a worthwhile trick that every surgeon should have in his or her armamentarium. It helps to reduce or retard the development VAO in pediatric eyes without the need for anterior vitrectomy, and it locks the IOL into its position within the capsular bag.
1. Apple DJ, Solomon KJ, Tetz MR, et al. Posterior capsule opacification. Surv Ophthalmol. 1992;37:73-116.
2. Koch DD, Kohnen T. A retrospective comparison of techniques to prevent secondary cataract formation following posterior chamber intraocular lens implantation in infants and children. Trans Am Ophthalmol Soc. 1997;95:351-360.
3. McDonnell PJ, Zarbin MA, Green WR. Posterior capsule opacification in pseudophakic eyes. Ophthalmology. 1983;90:1548-1553.
4. Plager DA, Yang S, Neely D, et al. Complications in the first year following cataract surgery with and without IOL in infants and children. J AAPOS. 2002;6:9-14.
5. Trivedi RH, Wilson ME Jr, Bartholomew LR, et al. Opacification of the visual axis after cataract surgery and single acrylic intraocular lens implantation in the first year of life. J AAPOS. 2004;8:156-164.
6. Lambert SR, Lynn M, Drews-Botsch C, et al. A comparison of grating visual acuity, strabismus, and reoperation outcomes among children with aphakia and pseudophakia after unilateral cataract surgery during the first 6 months of life. J AAPOS. 2001;5:70-75.
7. BenEzra D, Cohen E. Posterior capsulectomy in pediatric cataract surgery: the necessity of a choice. Ophthalmology. 1997;104:2168-2174.
8. Buckley EG, Klombers LA, Seaber JH, et al. Management of the posterior capsule during pediatric intraocular lens implantation. Am J Ophthalmol. 1993;115:722-728.
9. Vasavada A, Desai J. Primary posterior capsulorhexis with and without anterior vitrectomy in congenital cataracts. J Cataract Refract Surg. 1997;23:645-651.
10. Gimbel HV, DeBroff BM. Posterior capsulorhexis with optic capture: Maintaining a clear visual axis after pediatric cataract surgery. J Cataract Refract Surg. 1994;20:658-664.
11. Gimbel HV. Posterior continuous curvilinear capsulorhexis and optic capture of the intraocular lens to prevent secondary opacification in pediatric cataract surgery. J Cataract Refract Surg. 1997;23:652-656.
12. Raina UK, Gupta V, Arora R, Mehta DK. Posterior continuous curvilinear capsulorhexis with and without optic capture of the posterior chamber intraocular lens in the absence of vitrectomy. J Pediatr Ophthalmol Strabismus. 2002;39:278-287.
13. Vasavada A, Desai J. Primary posterior capsulorhexis with and without anterior vitrectomy in congenital cataracts. J Cataract Refract Surg. 1993;23:645-651.
14. Vasavada AR, Trivedi RH. Role of optic capture in congenital cataract surgery and intraocular lens implantation in children. J Cataract Refract Surg. 2000;26:824-831.
15. Koch DD, Kohnen T. Retrospective comparison of techniques to prevent secondary cataract formation after posterior chamber intraocular lens implantation in infants and children. J Cataract Refract Surg. 1997;23:657-663.
16. Menapace R. Posterior capsulorhexis combined with optic buttonholing: an alternative to standard in-the-bag implantation of sharp-edged intraocular lenses? A critical analysis of 1000 consecutive cases. Graefes Arch Clin Exp Ophthalmol. 2008;246:787-801.
17. Argento C, Badoza D, Ugrin C. Optic capture of the AcrySof intraocular lens in pediatric cataract surgery. J Cataract Refract Surg. 2001;27:1638-1642.
18. Chen MS, Ye YJ, Wang Y, et al. Posterior continuous curvilinear capsulorhexis with optic capture of the posterior chamber intraocular lens in pediatric cataract [in Chinese]. Zhonghua Yan Ke Za Zhi. 2006;42:400-402.
19. Chang S. LXII Edward Jackson Lecture: Open angle glaucoma after vitrectomy. Am J Ophthalmol. 2006;141:1033-1043.
20. Tassignon MJ, Gobin L, Mathysen D, et al. Clinical outcomes of cataract surgery after bag-in-the-lens implantation following ISO standard 11979-7:2006. J Cataract Refract Surg. 2011;37:2120-2129.
21. Grieshaber MC, Pienaar A, Stegmann R. Posterior vertical capsulotomy with vertical entrapment of the intraocular lens in congenital cataracts – prevention of posterior capsule opacification. J Cataract Refract Surg. 2005;31:886-894.
22. Vasavada AR, Vasavada VA, Shah SK, et al. Postoperative outcomes of intraocular lens implantation in the bag versus posterior optic capture in pediatric cataract surgery. J Cataract Refract Surg. 2017;43:1177-1183.

