
Not all of my cataract surgeries end with an intact posterior capsule, but by no means does this indicate that a complication occurred. The most common reasons I choose to perform posterior capsulorhexis on select patients are to avoid the need for future Nd:YAG posterior capsulotomy, to achieve the best optical performance, and to stabilize the IOL. Techniques for performing posterior continuous curvilinear capsulorhexis (PCCC) are discussed elsewhere in this cover focus, so I will forgo detailing those here. This article discusses when I choose to use PCCC and a related technique, posterior optic capture (POC).
AVOIDING LASER
Once I became adept at performing PCCC, I began to apply it to avoid the need for Nd:YAG laser posterior capsulotomy at a later date in certain patient populations. In my view, candidates for PCCC include those with severe kyphosis, scoliosis, and other physical limitations that inhibit proper positioning at a slit lamp; those with neurologic diseases such as amyotrophic lateral sclerosis, nystagmus, or significant tremor that could encumber laser treatment; and those with dementia or other mental incapacity that prevents adequate cooperation. Morbid obesity is also a relative indication, in my opinion. Essentially, if I have to use a portable slit lamp for the preoperative examination, I consider adding a PCCC to the treatment plan for cataract surgery.
Another group of patients in whom I use primary PCCC are those with significant posterior capsular plaques. I often choose to open the posterior capsule in a controlled fashion in these patients with a PCCC, rather than risk a posterior capsular tear during aggressive polishing. This group includes patients with posterior polar cataracts, as polishing the thin posterior capsule in these eyes to remove any remaining lens material can lead to rupture.
When I am implanting a presbyopia-correcting IOL in a patient with a posterior capsular plaque, I employ PCCC to impart the best visual performance at the earliest possible time. Also, because the posterior capsular opening is continuous, I feel confident that an exchange will be possible if the patient is dissatisfied or there are IOL power issues.
OPTIC CAPTURE
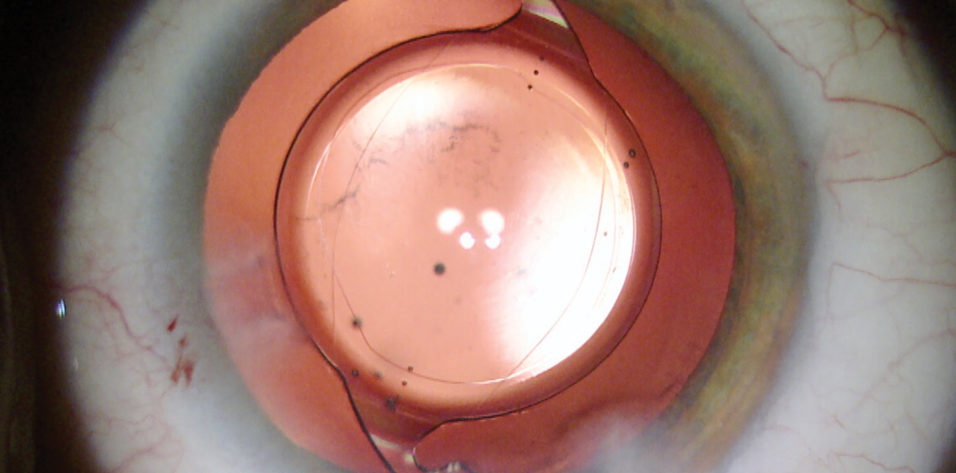
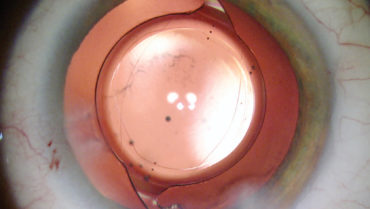
As I gained experience and improved my ability to control the size and shape of PCCCs, I recognized that capturing the IOL through the PCCC could be a valuable tool. This technique, POC, effectively maintains a clear visual axis and ensures excellent stability of the lens. I have used POC secondarily to treat a rotated toric IOL as well as primarily to avoid such rotation (Figure).
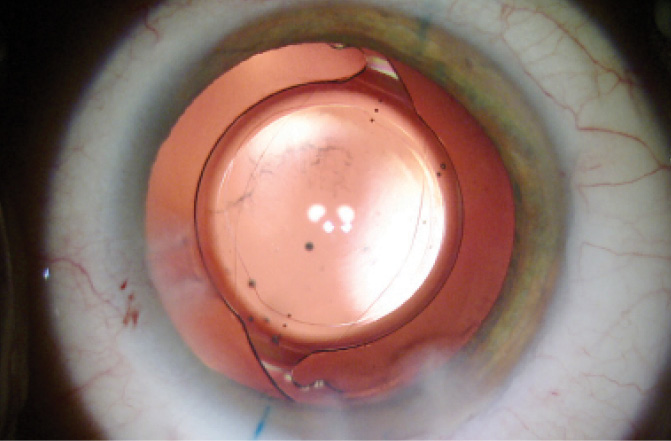
Figure. This one-piece acrylic toric IOL was secured in position with POC through a PCCC.
I have also used a double optic capture technique, with POC of a toric IOL and optic capture through the anterior capsulorhexis of a minus-powered three-piece IOL with haptics in the sulcus, to address high myopia and high astigmatism while maintaining excellent stabilization of the two lenses (bit.ly/0119Jones).
ONE-PIECE ACRYLIC
Which lens types are best to use with POC? I prefer to use one-piece acrylic posterior chamber IOLs for several reasons: I have significant experience with this style of IOL, the profile of the lens is low and requires little manipulation, the acrylic material allows great control for positioning, and this style of lens offers the greatest number of options in terms of technologies to benefit patients. Therefore, I can maintain all the benefits of a one-piece lens platform (potential for toric, presbyopic, and aspheric correction; routine incision and injector system) and marry those qualities to the advantages of PCCC. I have performed POC with one-piece IOLs from Alcon, Johnson & Johnson Vision, and Hoya with success, and I would expect any one-piece open-loop haptic IOL to perform well.
CONCLUSION
The dogma that the posterior capsule must be intact for a successful surgical outcome in cataract surgery is not necessarily true. There are distinct advantages in certain situations to performing PCCC with or without POC. Fortunately, there are excellent resources to learn the techniques of PCCC and POC, and I encourage all anterior segment surgeons to become familiar with these useful tools.