Capsulorhexis creation has been called both the most challenging and the most crucial step in phacoemulsification.1,2 A properly constructed capsulorhexis serves as the foundation for lens extraction and stable in-the-bag IOL fixation, but an errant capsulorhexis or an anterior capsular tear will compound the difficulty of each subsequent step of the procedure. Anterior capsular tears are particularly significant because they may extend to the equator and beyond. The mean incidence of anterior tears with manual capsulorhexis has been reported to be 2.3%, with a range as high as 5.1% among trainees.3,4
A properly sized continuous curvilinear capsulorhexis (CCC) allows the capsular bag to completely overlap the IOL optic, reducing the incidence of posterior capsular opacification. Histopathologic observations suggest that creating a CCC with a diameter slightly smaller than that of the IOL optic allows the edge of the capsule to adhere to the anterior surface of the optic, creating a closed system that enhances the efficiency of the barrier effect. However, in order to ensure that the anterior capsule overlaps the IOL edge by 360º after implantation, a manual CCC must be created with an average diameter somewhat smaller than ideal because of unavoidable variations in centration, diameter, and circularity.5 In clinical practice, where a range of surgical expertise is found, Findl reported 18% of cases with no rhexis overlap of the IOL.6
Beyond the safety implications of basic capsulorhexis sizing and location, there is new evidence that a perfectly centered, round capsulotomy results in less IOL tilt and decentration and a more predictable effective lens position, leading to more accurate refractive results.7 Although patients today can opt for femtosecond laser cataract surgery in conjunction with premium IOL upgrades, there remains a need for a simpler, safer, more cost-effective, and more predictable solution so that all surgeons can construct the ideal capsulotomy every time. Continuous thermal capsulotomy may offer such a solution. With the ApertureRx Continuous Capsulotomy System (International BioMedical Devices), thermal power is delivered through a microincision-compatible ring.
THERMAL CAPSULOTOMY
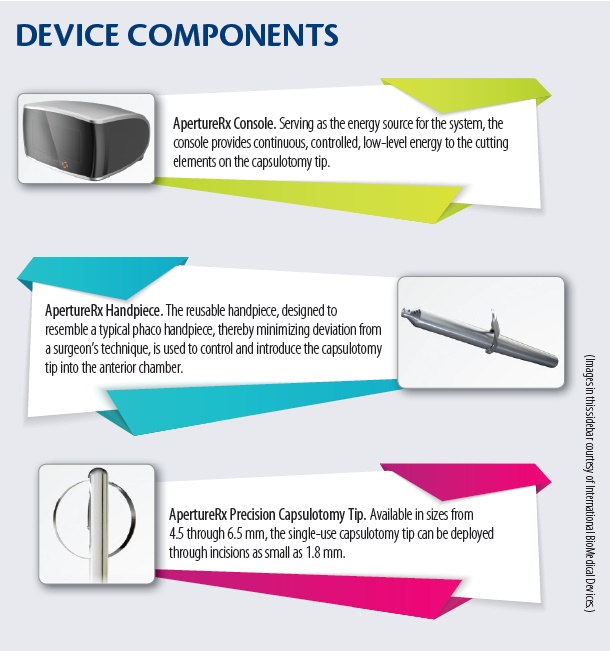
The 360º ring, which extends from an ergonomic handpiece, allows uniform contact with the anterior capsule (Figure). The procedure can be completed in milliseconds under the protection of an ophthalmic viscosurgical devices. As the ring is retrieved, it automatically captures and removes the perfectly circular cap. The disposable tip is discarded after the case, and the reusable handpiece is sterilized in standard fashion. For more information on the components of the ApertureRx, see Device Components.
The key features of the ApertureRx are its continuous 360º thermal element, which overcomes the inevitable gap required by radiofrequency devices with loop wire or ring cutting elements, and its uniform contact with the anterior capsule, which obviates the necessity for vacuum suction. This technology has the potential to ensure safer cataract surgeries and may also provide more predictable visual outcomes for patients.
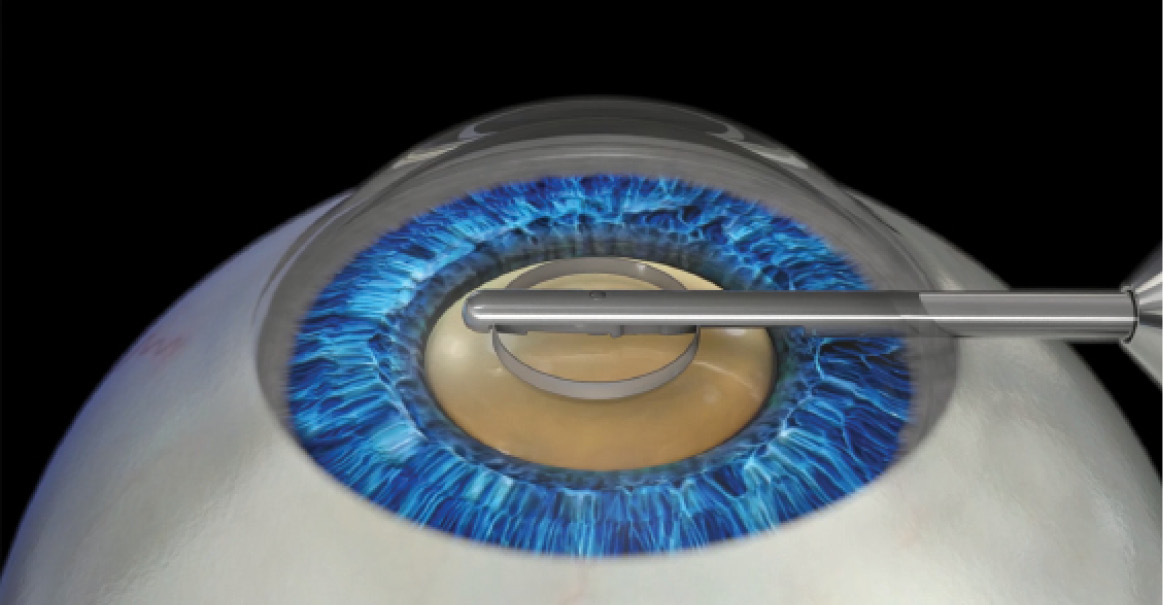
Figure. The 360° ring extends from an ergonomic handpiece and allows uniform contact with the anterior capsule.
CONCLUSION
By simplifying the current manual CCC procedure, the ApertureRx may allow a broader range of surgeons throughout the world to construct the capsulotomy with precise placement and a high degree of consistency. The ApertureRx Continuous Capsulotomy System has not been cleared or approved for use in Europe or the United States. After preclinical studies are complete, we surgeons can look forward to initiating clinical trials of the ApertureRx technology. n
1. Dooley IJ, O’Brien PD. Subjective difficulty of each stage of phacoemulsification cataract surgery performed by basic surgical trainees. J Cataract Refract Surg. 2006;32:604-608.
2. McCannel CA, Reed DC, Goldman DR. Ophthalmic surgery simulator training improves resident performance of capsulorhexis in the operating room. Ophthalmology. 2013;120(12):2456-2461.
3. Abell RG, Davies PE, Phelan D, Goemann K, McPherson ZE, Vote BJ. Anterior capsulotomy integrity after femtosecond laser-assisted cataract surgery. Ophthalmology. 2014;121(1):17-24.
4. Unal M, Yücel I, Sarici A, et al. Phacoemulsification with topical anesthesia: Resident experience. J Cataract Refract Surg. 2006;32(8):1361-1365.
5. Davidorf JM. Impact of capsulorrhexis morphology on the predictability of IOL power calculations. Paper presented at: American Academy of Ophthalmology Annual Meeting; November 11, 2012; Chicago, IL.
6. Findl O. Influence of rhexis size and shape on post-operative IOL tilt, decentration and anterior chamber depth. Paper presented at: European Society of Cataract and Refractive Surgeons Annual Meeting; October 5-9, 2013; Amsterdam, Netherlands.
7. Packer M, Teuma EV, Glasser A, Bott S. Defining the ideal femtosecond laser capsulotomy. Br J Ophthalmol. 2015;99(8):1137-1142.
Mark Packer, MD, CPI
• Mark Packer MD Consulting, Boulder, Colorado
• mark@markpackerconsulting.com
• financial disclosure: chief medical officer (International BioMedical Devices)