
Every patient knows cataract surgery is 100% successful, entails no discomfort, and is followed by immediate visual recovery, right? By this question, I am suggesting that your perspective on OR safety as a surgeon is quite different than your patients'. Torn posterior capsules, mangled irides, dropped nuclei, and endothelial decompensation make me lose sleep. Patients, however, would categorize these concerns as problems in surgery. Preoperatively, they worry instead about how they will see while awaiting surgery on their second eye, how they will instill drops, whether they will feel nauseated from sedation, etc. Postoperatively, they feel anxious about the speed of visual recovery, annoying symptoms such as dryness and dysphotopsia, and residual refractive error and unaided visual acuity.
How do you alter the surgical environment to improve the consistency of outcomes for your patients? My perspective on this matter changed completely after I stopped using a sharp phaco needle 10 years ago. The difference is a reduction in the number of random unwanted events. I emphasize the word random, because who can determine when complications will arise? Once the damage occurring from incidental or inadvertent contact with the iris or capsule is eliminated, patterns start to emerge for the rest.
No matter how surgically skilled you are, vision-threatening events can occur. Some contributing factors appear to be inconsequential but, in hindsight, had a huge bearing. This article briefly covers these incidentals—the “how did I get here” of complications—and the broader steps I have taken to reduce their occurrence.
IT BEGINS IN THE OFFICE
This discussion is outside the scope of the article, but I will summarize it in this way: there are no stupid questions or comments. Their timing may be inconvenient, but patients' questions and comments have the potential to improve the outcome. I find it can help to ask patients what made them think of a question, especially if it is not one I routinely encounter.
THE ADMINISTRATIVE PERSPECTIVE
Once the surgical day has begun, no one is to ask me about any paperwork that he or she does not have in hand to show me. Did I forget to sign a permit? That happens, and I am happy to sign it. Were the history and physical examination not received? There is no excuse for not accounting for the paperwork prior to the day in the OR. To a great extent, the success or failure of this step is a testimonial to a center's dedication to surgery. After all, the plan for the patient was included in that information. Does the staff not want to be prepared for that plan?
10 PEARLS
No. 1. Shield the Nonoperative Eye
The site is positively marked. A plastic shield is taped over the opposite eye to negatively mark the nonoperative site. This prevents a drop from accidentally reaching the nonoperative eye and reduces the potential for worse. (For a video illustrating Dr. Dewey's pearls, go to http://eyetube.net/?v=olafe.)
No. 2. Reduce Unexpected Movement
To decrease the risk of coughing, every patient receives 100 mg sodium benzonate (Tessalon Perles [Pfizer], Zonatuss [Vertical Pharmaceuticals]) in the preoperative suite. Rather than screen for snoring, sleep apnea, and so forth, it is easier to give this drug to everyone. This measure reduces unexpected axial movement at inconvenient times during surgery.
On the table, the patient needs to be properly positioned in as consistent a fashion as possible. Not only does this include comfortably addressing any neck and back issues he or she has, but more importantly, it entails establishing a reproducible height for the eye relative to the preferred surgical approach. An inconvenient position may seem trivial for one case, but it increases the risk of adverse events over the course of a series of cases.
Once positioned, every patient's head is taped to the bed. I use 2-inch wide paper tape, which only contacts about ¾ of an inch of the forehead, just below the surgical cap, usually 3 to 4 inches across. The head should be taped either with the nose vertical or with just a slight tilt toward the operative side; these configurations allow irrigating fluid to drain from the field.
My patients seem to appreciate how the tape helps them to hold still through the surgery. Taping will not eliminate all movement, but it lessens the magnitude of lateral head movement and allows instruments to be withdrawn safely if excessive movement is encountered.
No. 3. Use Temporal Positioning
In retrospect, I consider the superior approach to cataract surgery to be the single highest risk for complications I had yet to address. Because it is also the “standard” approach to cataract surgery, I did not come to this realization for awhile.
With the superior approach, the brow places the handpiece in an awkward position. You can tip the head as far back as possible, but does this chiropractic maneuver improve the situation that much? If so, for how long? Sudden movement during surgery is mainly due to coughing, which will affect the superior more than a temporal approach. Coughing will drive instruments farther into the eye or cause their unplanned, sudden withdrawal.
In addition, I have found that the superior approach results in a more poorly constructed incision and intraocular contortion during removal of the nucleus and implantation of the IOL. An adjustment to the astigmatism algorithm will be required if you counted on a superior incision to assist with the treatment of with-the-rule astigmatism.
No. 4. Perform Intracameral Dilation
All of my patients receive a compounded mix of nonpreserved epinephrine and lidocaine (“epi-Shugarcaine”) injected through the sideport at the beginning of the case (Figure 1). The premise is that every patient is at risk of intraoperative floppy iris syndrome. That is not the case. Assuming that every eye has the potential to surprise you with a poorly toned iris that is trying to prolapse out of the incision, however, means that you will encounter fewer surprises.
If you do not think this measure helps, use it for about a hundred cases. Then stop. After you compare your complication rates and the subjective ease of surgery, I bet that you will go right back to using it.
No. 5. Use Viscoelastics Carefully
Every staff member needs to understand that the safety hubs on the viscoelastic syringes are not for decoration. Ejecting a syringe is a rare and disastrous event but a preventable one.
Perform viscomydriasis on every patient. It traps the iris to the anterior capsule for the capsulorhexis and helps to stabilize the peripheral iris during phacoemulsification.
Never overfill a capsule with viscoelastic prior to inserting the IOL. The excessive pressure created during insertion can split the capsule with only minor contact by the IOL.
No. 6. Size the Primary Incision Appropriately
No patient judges the surgical result by the size of the incision. Make the primary incision as large as it needs to be for you to easily insert the phaco needle, prevent “oarlocking,” and implant the IOL without stretching the wound. Ensure adequate irrigation to avoid thermal injury and improve chamber stability. A well-constructed incision will allow self-sealing and provide consistent refractive results as well.

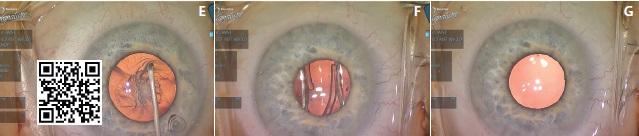
Figure 1. Intracameral dilation and viscomydriasis. Starting size during creation of the incision (A) and after intracameral dilation (B). Starting (C) and later (D) viscomydriasis. Size well suited to capsulorhexis (E). Implantation of the IOL (F). Without the support of viscoelastic, the pupil returns to its initial size by the end of the case (G).
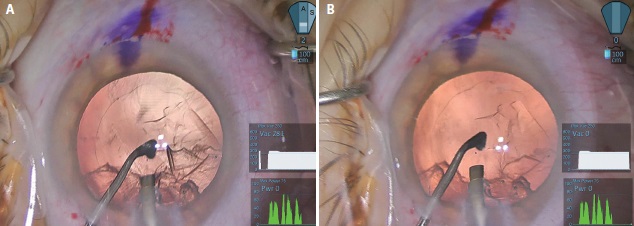
Figure 2. The capsule is incidentally engaged during cortical removal (A). Reflux shows an intact capsule (B). A “random” complication was avoided.
No. 7. Consider Instrumentation
The Dewey Radius Tip (MicroSurgical Technology) has changed how I perform surgery. I find this needle easy to use intraoperatively. I can work closer to the iris and capsule with higher vacuum and flow than I ever could with a sharp tip (Figure 2).
I find the instrument's design easy to use: any needle configuration with a highly polished, rounded edge. The tip is labeled for 20 uses. It works on any phaco unit—those from Abbott Medical Optics and Bausch + Lomb without fluidic changes and that of Alcon with minor tweaks to the fluidics. The instrument should not necessitate a change in your technique, but it will require gentle handling by the instrument cleaning team.
Does using this needle mean the end of broken capsules? Of course not, but in my hands, it has prevented a lot of problems that would have occurred if a sharp edge had been present. I am referring to cases involving high myopia, toric IOLs, and multifocal lenses and all of the problems that follow if the posterior capsule is not intact.
No. 8. Try a Smaller-Gauged Needle
A large-gauge needle (eg, 19 gauge) will use less power to remove a cataract, but that difference is trivial compared to the improved chamber stability it also brings. The benefits of a smaller incision are obvious: less induced astigmatism. A smaller needle also acts as a surge suppressor, reducing the potential for postocclusion surge regardless of the inherent benefits of current phaco technologies.
No. 9. Pay Attention to Irrigation Flow
Rotate the irrigation ports on the irrigating sleeves to direct flow away from the corneal endothelium, even when this means removing the tip to reorient the sleeve. Be especially careful in eyes with dense cataracts, shallow anterior chambers, and Fuchs dystrophy, because this misdirected flow can have a more significant impact.
No. 10. Alternate Cortical Removal
Nothing is more frustrating than subincisional cortex in an eye with an unstable anterior chamber and a prolapsing iris. Whether you use them routinely or not, have a set of bimanual I/A handpieces available. Practice on a stable eye for that unfortunate eventuality.
CONCLUSION
The rate of complications in cataract surgery is low enough to make analysis of the associated causes a challenge. It is not low enough, however, that you or I should be satisfied with current levels. A careful deconstruction of processes can identify the errant steps for correction.n
Steven Dewey, MD
• Pinnacle Eye Center, Colorado Springs, Colorado
• (719) 473-4507; deweys@prodigy.net
• consultant to Abbott Medical Optics
• receives royalties from MicroSurgical Technology for the Dewey Radius Tip

