



My passion for medical missions, or the delivery of eye-related health care to developing nations, began shortly after completing my medical training. My first experience, during an internship in 1997, was to staff a general medical clinic in a small Mayan village in the western part of Southern Belize. My husband and two daughters, aged 5 and 7 years, accompanied me. I spent 1 month in the rural community, pumping water from the well, washing clothes in the river, and providing basic medical care at the clinic, while my daughters attended the local school. This experience made a lasting impression on all of us. It broadened my children’s view of the world, and it sparked an interest in me to continue to provide medical eye care in developing countries.
I have amassed 2 decades of experience in medical mission work. My view on how to be most effective in improving eye care delivery to developing nations has evolved over time. Early in my career, like many ophthalmologists, I focused my time and energy on honing my clinical and surgical skills to provide the best care to the patient in my chair or on the stretcher. My field of view was limited mostly to the individual patient and my impact on their health at that moment. Today, my field of view has expanded to include teaching, research, leadership in professional societies, regulatory and legislative advocacy, and innovation and investment.
Expanding one’s view occurs naturally in the setting of medical missions. Those involved with mission work often find that their early activities focused on the number of patients treated over the course of the trip. Over time, their activities often evolve to include other pursuits such as teaching, mentoring, innovating, and advocating. The goal is to support sustainable expansion and continuity of high-quality care by local doctors.
The authors of the articles in this cover focus have all found ways to create long-term relationships with local providers, which is essential to improving the quality and quantity of care in developing countries. They have done this not only by teaching, mentoring, and sharing their expertise but also by providing access to capital equipment and supplies.
Some of the greatest challenges and opportunities for growth in my career have occurred during medical missions. Dennis, a young boy Timothy Page, MD, speaks about in his article (see pg 68), was the first patient I met on a trip to Kenya 5 years ago. Dennis’ story and others like his are heartbreaking. On my most recent medical mission to Kenya this August, I met a 4-year-old named Paul, who presented in terrible pain after trauma from a stick to his left eye 4 weeks earlier resulted in a full-thickness scleral perforation and endophthalmitis. Unfortunately, the injury required enucleation. Blinding cataracts (Figure at outset) and glaucoma, advanced melanoma of the conjunctiva, orbital tumors, squamous and basal cell carcinomas, and untreated sequelae of ocular and orbital trauma (Figures 1 and 2) are all reminders of how important access to care is in underserved, developing communities.
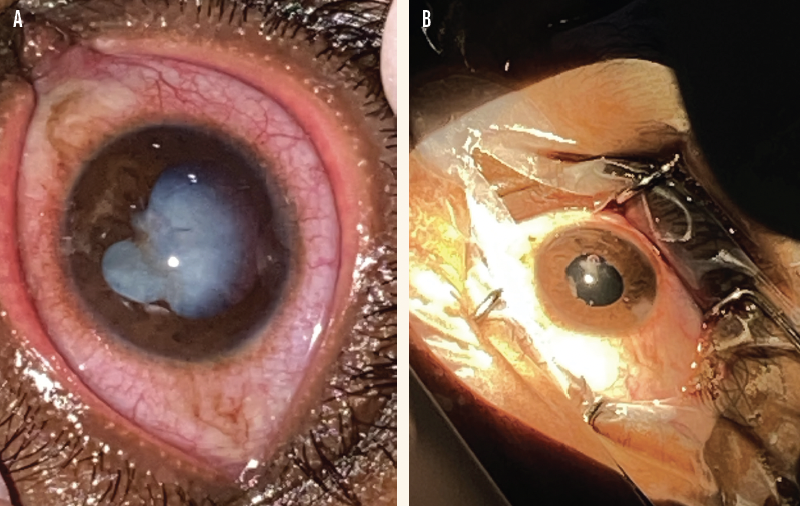
Figure 1. A 32-year-old man presented with a mature white cataract from an Acacia thorn injury to the left eye that penetrated the cornea, iris, and anterior and posterior capsular bags (A). Surgery without access to vitrectomy resulted in normal pupil contour, placement of a posterior chamber IOL, and restoration of vision (B).

Figure 2. A young boy underwent anterior chamber washout, cataract removal, and vitrectomy with a battery-powered handheld vitrector. He had been hit in the eye with a rock thrown by his brother 1 week prior and presented with a ruptured anterior capsule, a blood-filled anterior chamber, and an IOP of 50 mm Hg. In the figure, Dr. McCabe’s daughter Casey and son Max help move the patient at the end of surgery.
In a country such as Kenya, where more than 30 distinct languages and dialects are spoken, communicating with patients effectively presents another unique challenge. On one occasion, a small-but-mighty elderly Kenyan woman reached up, removed the drape and lid speculum from her eye, and jumped off the surgical table in the middle of small incision extracapsular cataract surgery. I think my heart stopped during the 10 to 15 minutes it took to find her nephew—the only person who spoke her dialect—and complete the surgery.
Performing challenging surgeries with limited resources requires flexibility and creativity, and learning such skills translates to improved surgical outcomes back at home. I have learned many tricks from other visiting surgeons and local ophthalmologists who have found inventive ways around limitations—necessity ignites intraoperative ingenuity. In this cover focus, Dr. Page and Eric Purdy, MD, FAAO, outline some of the creative solutions they developed during medical missions. Their solutions to replace burnt-out light bulbs and perform safer cortical cleanup work brilliantly, as does using sharp intraocular scissors as a substitute vitrector—something I learned from a local doctor in St. Vincent.
My family has participated in an annual medical mission to St. Vincent and the Grenadines since 2003. Dr. Purdy invited me initially; we continue to deliver surgical and clinical eye care and to distribute glasses in conjunction with local ophthalmologists who provide indigent care and with the local Lions Club. Like the surgeons in this cover focus who have participated in medical missions to Honduras, Tanzania, Nepal, and Kenya, Dr. Purdy and I have a longstanding relationship with the community and the doctors. We are expanding our efforts and have purchased a building to provide education, improved access to surgery time and equipment for local doctors, and provided more frequent mentoring and surgical missions. Additionally, our nonprofit organization, Sight for Life (Figure 3), was established to expand our impact on the region. Additionally, our nonprofit organization, Sight for Life, was established to expand our impact on the region. To learn more, and see Sight for Life in action, scan the QR code in Figure 3.
Figure 3. Sight for Life was established to expand the impact of Drs. McCabe and Purdy’s work in St. Vincent and the Granadines.
I look forward to learning from and partnering with the dedicated physicians who contributed to this issue; the organizations they have joined forces with are listed in the sidebar Get Involved!. I hope you are as inspired as I am by the advice and experiences they share.
Get Involved!
- ACE Global
acecaresglobal.org - Arunodaya Charitable Trust
www.adeh.in - ASCRS Foundation
ascrs.org/foundation/operation-sight - Central American Eye Clinics
aecosurgery.org/gc - Eye Corps
eyecorps.org - Hawaiian Eye Foundation
hawaiianeyefoundation.org - Himalayan Cataract Project
www.cureblindness.org - John A. Moran Eye Center Global Outreach Division
healthcare.utah.edu/moran/outreach - Kenya Relief
www.kenyarelief.org - Orbis International
www.orbis.org - Surgical Eye Expeditions
www.seeintl.org

