




I (DKD) can trace my interest in acupuncture’s potential ophthalmic indications back to 2004. After getting my department chair’s blessing to investigate the matter, my first step was to become a licensed acupuncturist through coursework at UCLA. Next, I founded the Center for Integrative Eye Care at the University of Pittsburgh. I have reviewed the research on the use of acupuncture for the treatment of dry eye disease (DED), and my colleagues and I are now studying whether we can validate a protocol that has been described. Admittedly, this is a Western approach to Eastern medicine.
MECHANISM OF ACTION
The roots of acupuncture are ancient. It is thought to have originated in China more than 3,000 years ago,1 and texts written during the Ming dynasty (1368–1644) outlined the foundations of the practice.2
Treatment involves inserting slender (0.12–0.35 mm) needles into the skin at specific points. In a typical session, the practitioner places needles in a set of acupoints that match a therapeutic goal. There are hundreds of acupoints in the body.
Acupuncture’s mechanism of action is unclear, but several hypotheses have been proposed. Treatment has been shown to decrease proinflammatory cytokines, suggesting applications for chronic inflammatory conditions such as DED.3,4 Acupuncture has also been found to reduce pain,5,6 increase blood flow to organs,7 and modulate the sympathetic nervous system. Electrically stimulating acupoints using needles connected to electrodes has been shown to enhance wound healing.8
SAFETY
When it is performed by physicians, acupuncture is relatively safe, but patients should be informed of the potential for adverse effects. Most of these are mild and transient. They include needling pain and bleeding or bruising at the needle site.
In a large prospective study, the incidence of minor adverse effects was 6.7%.9 Serious adverse effects have been associated with acupuncture in the abdominal and thoracic regions,2 but one study found them to be three times more common with acupuncturists who were not medically trained than with acupuncturists who were medically trained.10 In another prospective observational study of nearly 230,000 patients, 8.6% reported at least one adverse effect, and 2.2% reported experiencing at least one adverse effect that required treatment.11
AT A GLANCE
- The roots of acupuncture are ancient, and its mechanism of action is unclear.
- Several randomized controlled trials have shown that acupuncture produces statistically significant improvements in parameters of dry eye disease compared with artificial tears, but the effects are not immediate.
A GROWING BODY OF EVIDENCE
In an observational study of 50 patients, acupuncture produced a significant improvement in DED symptom scores, Ocular Surface Disease Index (OSDI) questionnaire scores, and Schirmer test scores. No change in tear breakup time (TBUT) was observed.12
In an animal model, treatment produced changes in tear protein expression and lacrimal gland function.13 In a human study, it resulted in a statistically significant increase in TBUT and lipid layer thickness but not in Schirmer II test scores.14 A meta-analysis of data from seven randomized controlled trials (RCTs) comparing acupuncture with artificial tears found that acupuncture improved TBUT, Schirmer I test scores, corneal fluorescein staining, and visual analogue scale scores.15
Another study randomly assigned patients with Sjögren and non–Sjögren syndrome DED and lipid tear deficiency to therapy with acupuncture or artificial tears.16 The investigators reported significant improvements in tear film parameters such as tear meniscus height, depth, and area as well as in OSDI, TBUT, and Schirmer I test values after acupuncture in the non–Sjögren syndrome DED and lipid tear deficiency groups but not in the Sjögren syndrome DED group. These findings suggest that acupuncture’s effects may vary depending on the type of DED and that this form of therapy may not benefit patients with Sjögren syndrome.
Traditional Chinese Medicine Offers a Quantum Perspective
By Mark Packer, MD, FACS, CPI

Traditional Chinese Medicine (TCM) provides a systematic and holistic approach to health and disease that has maintained its allure for modern scientific research. Within TCM, the principles of yin and yang represent countervailing and complementary aspects of physiology that are related, respectively, to inner and outer, contraction and expansion, dark and light. Practitioners diagnose imbalance and design therapeutic interventions based on ancient principles developed empirically over thousands of years. Treatment is individualized based on the patient’s constitution as well as signs and symptoms. For this reason, the application of clinical research principles to TCM is a challenge. Nevertheless, in the accompanying article, Deepinder K. Dhaliwal, MD, LAc, and Siwei Zhou, MD, highlight some promising findings that support continued research into the potential benefits of acupuncture therapy in dry eye disease.
Eastern philosophy informs the principles of TCM. In a foreword to a translation of the I Ching, or Book of Changes, Carl Jung wrote:
“The ancient Chinese mind contemplates the cosmos in a way comparable to that of the modern physicist, who cannot deny that his model of the world is a decidedly psychophysical structure.”1
Jung’s statement alludes to the Heisenberg uncertainty principle. It is worth noting that Niels Bohr, who won the Nobel Prize for physics in 1922, adopted the familiar dark-light yin-yang symbol, called the taichi or taijitu, and the motto Contraria sunt complementa (opposites are complementary) for his family crest (Figure).2 Bohr saw echoes of Eastern philosophy in the complementary opposites inherent in quantum mechanics. As opposed to the causal view of events that underlies Newtonian physics, the synchronistic world view of Eastern philosophy resembles modern physics in its rejection of causality: Both systems understand the universe as a constellation of concomitant events in order to elicit meaning from coincidence.

Figure. The family crest of Nobel Prize–winning physicist Niels Bohr.
Clinical research today has more in common with classical than modern physics. We clinicians examine the effectiveness of a specific treatment on a single disease entity in isolation (ie, we study cause and effect). A more holistic view might seek to discover all the determinants of a successful outcome in real time. We certainly adopt a more synchronistic point of view in our practical management of patients, for we recognize that satisfaction and success depend not only on the objective outcomes of surgery but also on the expectations we set, the office environment we create, and the quality of the human interaction our clinic staff provides.
In the future, we may be able to expand our notions of safety and effectiveness to encompass the whole patient experience of disease and health. The addition of patient-reported outcomes to clinical research projects represents a step in this direction, but current questionnaires tend to be quantitative and directed rather than qualitative and open-ended, thereby limiting their scope. It remains a challenge for ophthalmic clinical research to recognize and accept the significance of psychosocial factors in outcomes.
1. Jung CG. Foreword. In: Wilhelm R, Baynes CF, translators. The I Ching, or, Book of Changes. Bollingen Series XV. Princeton, NJ: Princeton UP; 1997:xxi-xxxix.
2. Escutcheons of Science. http://www.numericana.com/arms/bohr.htm. Accessed September 26, 2018.
Interestingly, several RCTs have shown that acupuncture produces statistically significant improvements in DED parameters compared with artificial tears—but not immediately.16-21 One study comparing acupuncture to treatment with artificial tears found significant differences in terms of patient symptoms, TBUT, and Schirmer test scores only after 3 weeks.19 Another study comparing the results of treatment with acupuncture or artificial tears found no differences immediately after treatment but significant improvements in the mean OSDI score and visual analogue scale score in the acupuncture group 8 weeks after treatment.18
Solid proof of acupuncture’s efficacy remains elusive because of the small number of RCTs, small sample sizes in studies, and lack of true negative controls. Few RCTs have used sham acupuncture treatment as a negative control, and it has been argued that sham acupuncture treatment itself can produce physiologic changes and thus cannot serve as a placebo control.22,23
Targeting Other Ophthalmic Conditions
Investigators have examined acupuncture for the treatment of glaucoma,1,2 retinitis pigmentosa,3 and age-related macular degeneration (AMD).4
At the Center for Integrative Eye Care at the University of Pittsburgh, we are conducting a pilot study of acupuncture for the treatment of dry AMD. Ten patients have been enrolled, and we are currently collecting 6-month data on the last of these patients, after which we will commence data analysis.
A few of the patients have experienced dramatic improvement, a few achieved minimal improvement, and some had no improvement. A few eyes did progress to exudative AMD, so we need to be cautious. These are early results from a small pilot study. We look forward to publishing our full results once data analysis has been completed.
1. Smith JR, Spurrier NJ, Martin JT, Rosenbaum JT. Prevalent use of complementary and alternative medicine by patients with inflammatory eye disease. Ocul Immunol Inflamm. 2004;12(3):203-214.
2. Law SK, Li T. Acupuncture for glaucoma. Cochrane Database Syst Rev. 2013:(5):CD006030.
3. Bittner A, Gould J, Rozanski C, et al. Visual function improvements following electroacupuncture for retinitis pigmentosa. Invest Ophthalmol Vis Sci. 2013;54(15):4017.
4. Lundgren AC. Medical acupuncture for age-related macular degeneration: a preliminary report. Medical Acupuncture. 2003;14(2):37-39.
OUR RESEARCH
The reported protocols for treating DED with acupuncture vary greatly. For that reason, we and our colleagues conducted a prospective, randomized, double-masked, sham acupuncture–controlled study using the Niemtzow protocol24 at the University of Pittsburgh (D.K. Dhaliwal, S. Zhou, M.K. Rhee, et al, unpublished data, 2016). The study enrolled 49 patients, each of whom received acupuncture on 2 consecutive days for a total of two treatments (Figure). We used the OSDI questionnaire, ocular surface staining, tear flow measurements, TBUT, and a general questionnaire to evaluate outcomes.
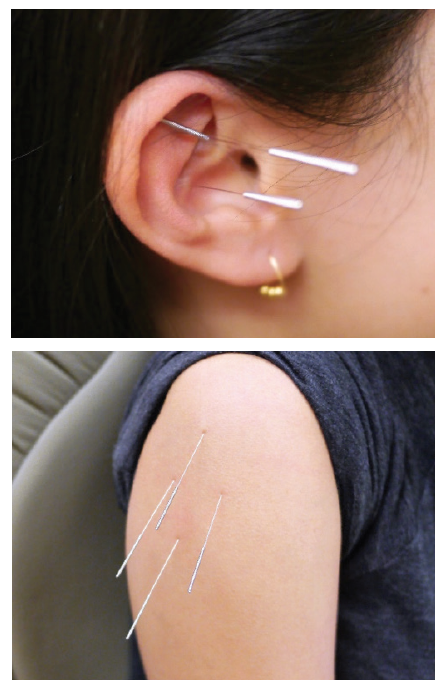
Figure. True (top) and sham (bottom) acupuncture therapy as used by Dr. Dhaliwal and colleagues in their study.
At 1 week, each patient group showed an improvement in mean OSDI score. At 6 months, the acupuncture group demonstrated a significant improvement in mean OSDI score compared with the sham group (P = .04). We observed no differences in TBUT, tear flow, or ocular surface grading between groups. Despite the lack of difference in objective DED measures, the patients in the acupuncture group reported symptomatic improvement lasting at least 6 months.
CONCLUSION
Traditionally, practitioners of Western medicine have been skeptical of Eastern medicine, but recognition of integrative medicine’s power and place is growing ever so slowly in the United States, as evidenced by the establishment of the National Center for Complementary and Integrative Health at the US National Institutes of Health. Acupuncture’s mechanisms of action are still poorly understood, but they may lie in decreasing inflammation and the sensation of pain through molecular pathways. The lack of a true negative control poses a challenge to the design of appropriately powered RCTs, but acupuncture’s relative safety and patients’ growing willingness to explore complementary medicine make the practice worth studying for the treatment of DED and other ophthalmic conditions (see Targeting Other Ophthalmic Conditions).
1. White A, Ernst E. A brief history of acupuncture. Rheumatology (Oxford). 2004;43(5):662-663.
2. Ernst E. Acupuncture—a critical analysis. J Intern Med. 2006;259(2):125-137.
3. Oke SL, Tracey KJ. The inflammatory reflex and the role of complementary and alternative medical therapies. Ann N Y Acad Sci. 2009;1172:172-180.
4. Kavoussi B, Ross BE. The neuroimmune basis of anti-inflammatory acupuncture. Integr Cancer Ther. 2007;6(3):251-257.
5. Bäcker M, Grossman P, Schneider J, et al. Acupuncture in migraine: investigation of autonomic effects. Clin J Pain. 2008;24(2):106-115.
6. Nepp J, Jandrasits K, Schauersberger J, et al. Is acupuncture a useful tool for pain-treatment in ophthalmology? Acupunct Electrother Res. 2002;27(3-4):171-182.
7. Uchida S, Hotta H. Acupuncture affects regional blood flow in various organs. Evid Based Complement Alternat Med. 2008;5(2):145-151.
8. Kloth LC. Electrical stimulation for wound healing: a review of evidence from in vitro studies., animal experiments, and clinical trials. Int J Low Extrem Wounds. 2005;4(1):23-44.
9. White A, Hayhoe S, Hart A, Ernst E. Adverse events following acupuncture: prospective survey of 32 000 consultations with doctors and physiotherapists. BMJ. 2001;323(7311):485-486.
10. Ernst E, White A. Life-threatening adverse reactions after acupuncture? A systemic review. Pain. 1997;71(2):123-126.
11. Witt CM, Pach D, Brinkhaus B, et al. Safety of acupuncture: results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch Komplementarmed. 2009;16(2):91-97.
12. Jeon JH, Shin MS, Lee MS, et al. Acupuncture reduces symptoms of dry eye syndrome: a preliminary observational study. J Altern Complement Med. 2010;16(12):1291-1294.
13. Qiu X, Gong L, Sun X, et al. Efficacy of acupuncture and identification of tear protein expression changes using iTRAQ quantitative proteomics in rabbits. Curr Eye Res. 2011;36(10):886-894.
14. Nepp J, Tsubota K, Goto E, et al. The effect of acupuncture on the temperature of the ocular surface in conjunctivitis sicca measured by non-contact thermography: preliminary results. Adv Exp Med Biol. 2002;506(pt A):723-726.
15. Yang L, Yang Z, Yu H, Song H. Acupuncture therapy is more effective than artificial tears for dry eye syndrome: evidence based on a meta-analysis. Evid Based Complement Alternat Med. 2015;2015:143858.
16. Lin T, Gong L, Liu X, Ma X. Fourier-domain optical coherence tomography for monitoring the lower tear meniscus in dry eye after acupuncture treatment. Evid Based Complement Alternat Med. 2015;2015:492150.
17. Zhang Y, Yang W. Effects of acupuncture and moxibustion on tear-film of the patients with xerophthalmia. J Tradit Chin Med. 2007;27(4):258-260.
18. Grönlund MA, Stenevi U, Lundeberg T. Acupuncture treatment in patients with keratoconjunctivitis sicca: a pilot study. Acta Ophthalmol Scand. 2004;82(3 pt 1):283-290.
19. Gong L, Sun X, Chapin WJ. Clinical curative effect of acupuncture therapy on xerophthalmia. Am J Chin Med. 2010;38(4):651-659.
20. Kim TH, Kang JW, Kim KH, et al. Acupuncture for the treatment of dry eye: a multicenter randomised controlled trial with active comparison intervention (artificial teardrops). PLoS One. 2012;7(5):e36638.
21. Nepp J, Wedrich A, Akramian J, et al. Dry eye treatment with acupuncture. A prospective, randomized, double-masked study. Adv Exp Med Biol. 1998;438:1011-1016.
22. Lund I, Näslund J, Lundeberg T. Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist’s perspective. Chin Med. 2009;4:1.
23. Lund I, Lundeberg T. Are minimal, superficial or sham acupuncture procedures acceptable as inert placebo controls? Acupunct Med. 2006;24(1):13-15.
24. Johnstone PA, Peng YP, May BC, et al. Acupuncture for pilocarpine-resistant xerostomia following radiotherapy for head and neck malignancies. Int J Radiat Oncol Biol Phys. 2001;50(2):353-357.

