



Topography-guided laser ablation is arguably the most effective approach to treating an irregular cornea, but it may also carry the challenge of programming the cylinder correction. Manifest and anterior corneal astigmatism are usually closely correlated in virgin eyes. The manifest astigmatism is typically used when programming the cylinder in both noncustomized and topography-guided treatments. When the cornea is irregular, however, the manifest and anterior corneal astigmatism often do not match because coma and other odd-order higher-order aberrations (HOAs) refract as astigmatism and in cases where the optical contribution of the posterior cornea is significant.
ODD-ORDER ABERRATIONS
The topography-guided ablation of irregular corneas always includes treatment of anterior corneal irregularities, which may complicate programming of cylinder correction in an unpredictable fashion. Hence, it is important to anticipate and understand the consequences of the morphologic changes caused by treatment on the postoperative corneal and manifest cylinder.
During manifest refraction, patients are presented with a combination of spherical and cylindrical lenses until the image projected onto the fovea comes into sharp focus. However, when the cornea is irregular, the image’s clarity may still be insufficient after correcting the spherical and cylindrical errors. This can be further improved by adjusting the corrective sphere and cylinder to partially correct the HOAs. However, this could lead to errors in estimating the true sphere and cylinder, potentially resulting in refractive surprises if the manifest sphere and cylinder are used when programming topography-guided treatments. The partial correction of the HOAs by means of spherical and cylindrical correction must therefore be considered when programming the topography-guided ablation of cylinder in eyes with irregular corneas.
The difference between the manifest astigmatism and the astigmatism measured by corneal topography has been ascribed to the contribution of coma-like HOAs and is directly influenced by their magnitude.1 My research group studied eyes with coma-dominant corneal optics and low lenticular astigmatism. The vectorial difference between the corneal and manifest astigmatism, or discrepant astigmatism, correlated well to the angle and amount of coma. We also found that vertical coma–like HOAs increased the manifest against-the-rule (ATR) astigmatism and decreased the manifest with-the-rule (WTR) astigmatism.
Topography-guided treatment removes the HOAs from the anterior corneal surface and their influence on the manifest astigmatism. In this situation, it is preferable to treat the topography-measured (vs manifest) astigmatism. When implanting a toric IOL, however, it may be a better strategy to target the manifest astigmatism because the corneal HOAs will be left untouched and their partial correction by the implant’s cylinder may be desirable.2
POSTERIOR CORNEAL ASTIGMATISM
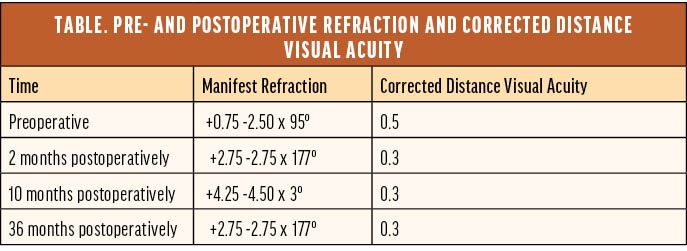
One of the first topography-guided procedures I performed was in 2005 with a LaserSight laser (LaserSight Technologies). The patient had undergone incisional surgery for high astigmatism in the mid-1990s and presented with serious visual disturbances, reduced visual acuity, and highly irregular corneal topography (Figure 1). Topographic data were obtained with an Orbscan (Bausch + Lomb) and exported to CIPTA ablation planning software (iVIS Technologies). The influence of the posterior corneal surface was not seriously considered at the time, so the programmed ablation pattern and simulated outcome appeared reasonable to me (Figure 2). The real postoperative anterior topography did as well (Figure 3). To the patient’s and my dismay, however, their vision deteriorated after surgery, and the amount of astigmatism more than doubled (-2.50 D ATR turned to -2.75 D WTR) and remained that way for years to come (Table).
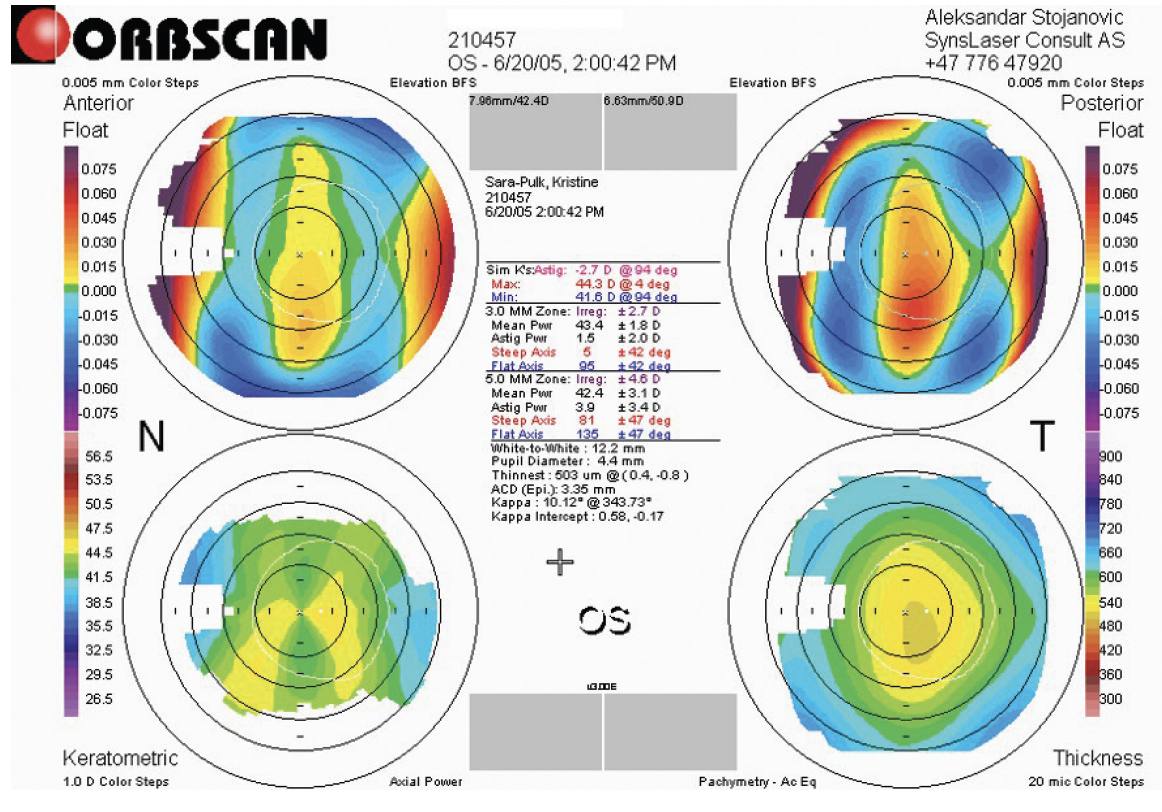
Figure 1. Preoperative Orbscan topography.
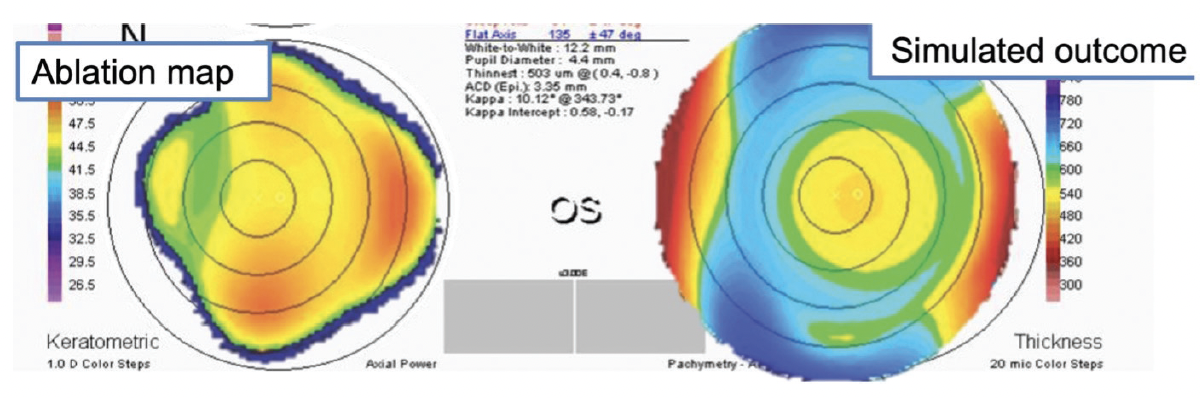
Figure 2. Topography-guided ablation plan and simulated outcome.
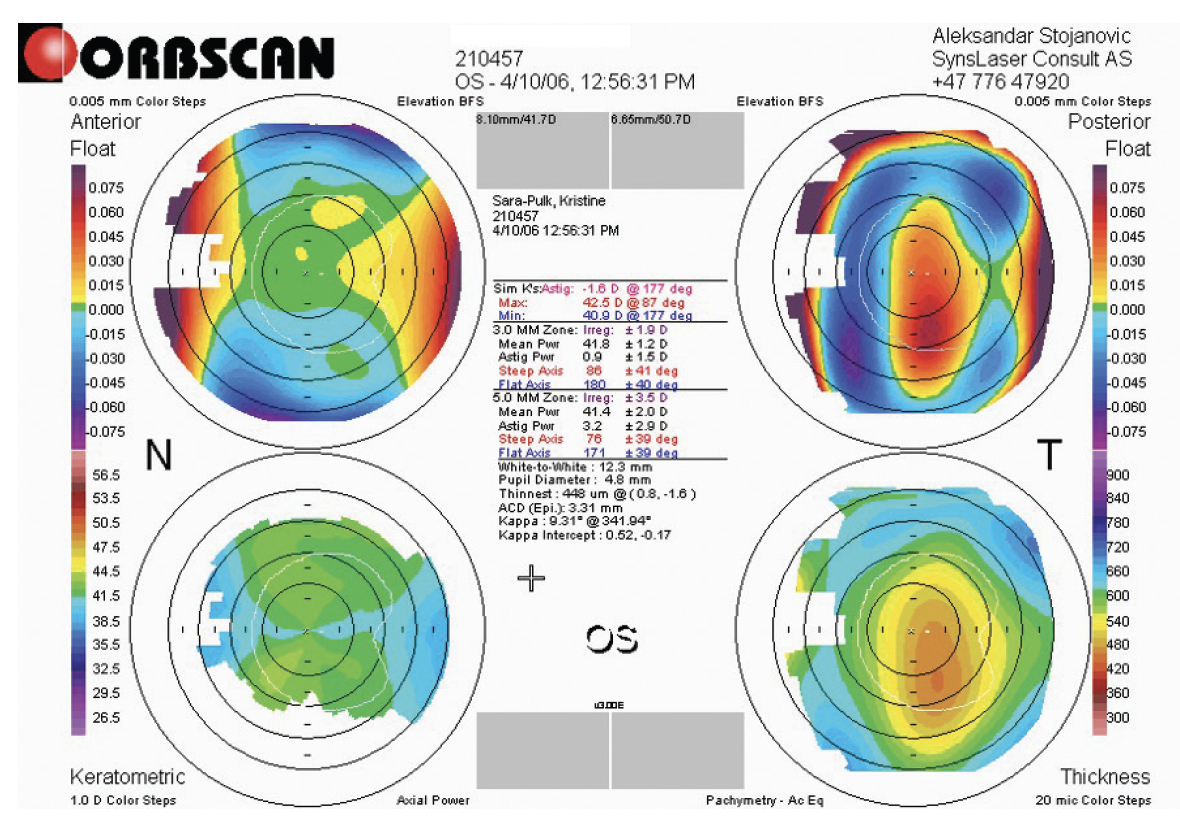
Figure 3. Postoperative Orbscan topography.
After an extensive evaluation and exclusion of all other possibilities, ATR posterior coma and ATR posterior corneal astigmatism were identified as the sources of the patient’s reduced vision and an overcorrection of the manifest astigmatism by more than 100% after regularization of the anterior cornea. I theorized that the significant posterior astigmatism and the coma had been preoperatively compensated for by their anterior counterparts and that the effects of the former became manifest after the anterior surface was regularized.
A couple years after the patient underwent surgery, two studies were published that described how major morphologic irregularities on the posterior corneal surface—especially in keratoconus—may be offset by equivalent irregularities (with the opposite optical effect) on the anterior corneal surface.3,4 The studies suggested that the dominant posterior corneal irregularities in keratoconic eyes are partially optically balanced by their less pronounced anterior counterparts and that regularization of the latter increases the optical contribution of the posterior corneal surface and degrades the optical quality. The investigators also referred to clinical results showing an increase in total ocular HOAs and poorer visual performance in some keratoconic eyes corrected by rigid gas permeable contact lenses.3,4 The situation is akin to treating the anterior corneal surface with topography-guided laser ablation.
WHAT TO DO?
The posterior cornea cannot be accessed surgically. The question, therefore, is how ophthalmologists should approach an eye in which posterior corneal irregularities are dominant, for example in keratoconus, where CXL combined with topography-guided laser treatment is often considered, or irregularity after incisional refractive surgery, where regularizing therapeutic refractive surgery is desired. The following five points should be considered:
No. 1. Anterior corneal topography–guided treatment should be avoided in these eyes.
No. 2. Wavefront-guided laser vision correction may be performed if there is confidence in the quality of the preoperative data. Unfortunately, confidence will often be lacking because of the limitations of technology for highly irregular corneas, prone to artifacts.
No. 3. Transepithelial phototherapeutic keratectomy (T-PTK), programmed to the depth of the thickest point of the epithelium, may be an option for these eyes because the T-PTK will leave a fair amount of the anterior corneal irregularities untreated and compensate for the posterior corneal irregularities.
No. 4. Noncustomized PRK may still be a better choice than the anterior corneal topography–guided treatment if the preoperative manifest astigmatism significantly improves vision. (For information on customized ablations, see the sidebar Technological Innovation.)
No. 5. Above all, treatment should not be performed if the surgeon is uncertain of its consequences on the total corneal optics.
Technological Innovation
Technologies that use ray tracing for customized ablation, such as Innoveyes (Alcon) and iVis Suite2 (iVIS Technologies), are designed to create irregularities on the anterior corneal surface that compensate for the optical effect of the posterior corneal higher-order aberrations. Innoveyes-guided ablation acquires posterior corneal data using classic Scheimpflug topography, which may not be ideal because the technology is prone to artifacts caused by stromal opacities.1 The iVis Suite2 uses novel ultrathin, blue laser light corneal imaging that the company claims yields a very high resolution of 120,000 points of the anterior corneal, stromal, and posterior corneal surfaces, which allows precise corneal ray tracing in irregular corneas.
1. Faria-Correia F, Ambrósio Júnior R. Clinical applications of the Scheimpflug principle in ophthalmology. Rev Bras Oftalmol. 2016;75(2):160-165.
1. Wei RH, Lim L, Chan WK, Tan DT. Higher order ocular aberrations in eyes with myopia in a Chinese population. J Refract Surg. 2006;22(7):695-702.
2. Zhou W, Stojanovic F, Reinstein DZ, et al. Coma influence on manifest astigmatism in coma-dominant irregular corneal optics. J Refract Surg. 2021;37(4):274-282.
3. Negishi K, Kumanomido T, Utsumi Y, Tsubota K. Effect of higher-order aberrations on visual function in keratoconic eyes with a rigid gas permeable contact lens. Am J Ophthalmol. 2007;144(6):924-929.
4. Marsack JD, Parker KE, Pesudovs K, Donnelly WJ 3rd, Applegate RA. Uncorrected wavefront error and visual performance during RGP wear in keratoconus. Optom Vis Sci. 2007;84(6):463-470.

