

J. Morgan Micheletti, MD, admits he has found his calling in ophthalmology, but perhaps for an unexpected reason: it provides his curious mind an outlet with which to tinker.
In a recent episode, Dr. Micheletti recalled being a kid who liked to take apart and put back together household appliances—sometimes with a few leftover screws. Now, he’s applied that inquisitiveness to the practice of ophthalmology. “Every step that I do, from cataract surgery to pterygium surgery, or anything we do in clinic or elsewhere, I say, 'Why am I doing this? Can this be done in a more efficient manner? How can we take what we have and improve upon it?'”
Lens Exchanges With Premium IOLs
Take, for example, Dr. Micheletti’s proposed modification on the twist and out technique, which was introduced in 2020 by Chapman et al.3 He told Dr. Singh that during one particular case where he was performing the technique, he had placed paracentesis incisions 180º apart, as is his practice. Just before he was about to ask for the spatula for his left hand, he changed his mind and asked for a 25-gauge cannula instead, just to try it. With the cannula threaded from the sideport to the secondary incision, he had bridged the gap and thereby provided structural support.
“Now I have a cannula bridging, going across the anterior chamber, protecting the endothelium, providing that mechanism to roll the IOL against,” he said.
Using the cannula for counter-traction, Dr. Micheletti could now use two hands to rotate the forceps and wrap the IOL before retracting it (Figure 1). He added that the technique was titratable, and that he performed it through a 2.4-mm incision or smaller. He also likes that the technique does not require extra instrumentation. During the episode, Drs. Micheletti and Singh reviewed a case video in which Dr. Micheletti demonstrated the modification.
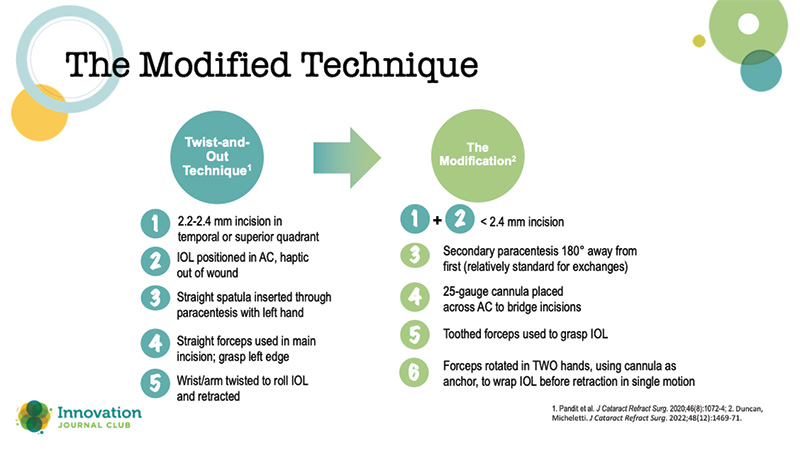
Figure 2. Dr. Micheletti's modified technique.
The Punch Technique
When an IOL is dislocated within the capsular bag, the standard of care is to extract it and implant a 3-piece IOL with scleral fixation. Often, premium IOL recipients don’t want the lens explanted. They’ve paid more for it, and they like the vision the IOL gives them. In these cases, Dr. Micheletti will present the patient the option of fixating the IOL. “If it's still floating on the interior hyaloid face, or just at least high enough up in the anterior chamber that I as an anterior segment surgeon can get to it, then I think it's worth the discussion with the patient.”
The particular technique Dr. Micheletti uses for these cases is a good example of inspiration striking when least expected (Figure 2). During the COVID lockdown, Dr. Michelletti was watching surgical videos on Eyetube, when he came across a video of Sergio Canabrava, MD, performing an external punch. A couple of days later, he was watching his kids use a hole puncher in paper cups. “And I was like, what if we took Dr. Canabrava's punch, and miniaturized it, and could use it in the eye?”

Figure 3. The punch and rescue technique.
He contacted his local ophthalmic company, Diamatrix, Ltd., in Houston, about his idea, and they developed a prototype within 2 weeks.
Initially, he used 5–0 prolene sutures,4 but now performs the technique with 6–0 or even 7–0 sutures, which he threads through the haptic-optic junction to secure the lens. “Basically, you're creating a rivet; a double flange. You're flanging one side with low-temp cautery, going through that hole that you've created inside the haptic-optic junction inside the eye. And that's what makes this unique: you're creating a hole inside the lens, inside the eye.” The surgeon removes the cored piece of the IOL from the punch device, docks the suture with a 25-gauge needle, and pulls it out, similar to haptic fixation. The step is repeated on the other side of the IOL.