



Office-based surgery centers are becoming the facilities of choice for some surgeons and their patients. These facilities allow tighter control of the surgical process from start to finish, including the patient experience, infection control protocols, and schedule density. Management of such factors has become critically important during the COVID-19 pandemic, which could lead to increased interest in these centers.
As surgeons all over the world navigate reopening their practices for elective surgery, those who have made the switch to an office-based facility can feel confident they are well positioned to manage the process.
ASC DRAWBACKS
Before we opened our office-based surgery center, I had been operating at an open-access ambulatory surgery center (ASC) for many years. It was a high-quality ASC, but several aspects were not ideal.
First, if a new device or technology became available, approval by committee was necessary before a purchase could be made. There were also ongoing challenges with surgery scheduling with multiple surgeons using the center. Billing for premium cataract surgery or cash-pay procedures such as refractive lens exchange or phakic IOLs was cumbersome and often led to patient confusion. And although the patient experience at that ASC was better than at just about any other outpatient surgery facility in our area, it was still not as good as the experience we could provide to LASIK patients who came to our office for their procedures. I noted a significant gap in patient satisfaction between our IOL patients and our LASIK patients.
SAFETY FIRST
Patient safety is, of course, the primary concern when considering a new surgical facility, and this is especially true amid the COVID-19 pandemic. Surgeons who are unfamiliar with office-based surgery centers often envision surgery being performed in a clean room or traditional procedure room, but that is not the case. Office-based surgery centers are full-fledged ORs, built and run with processes and protocols that are similar to or better than those at ASCs. Office-based centers can be fully accredited and require the same reporting and compliance processes as ASCs.
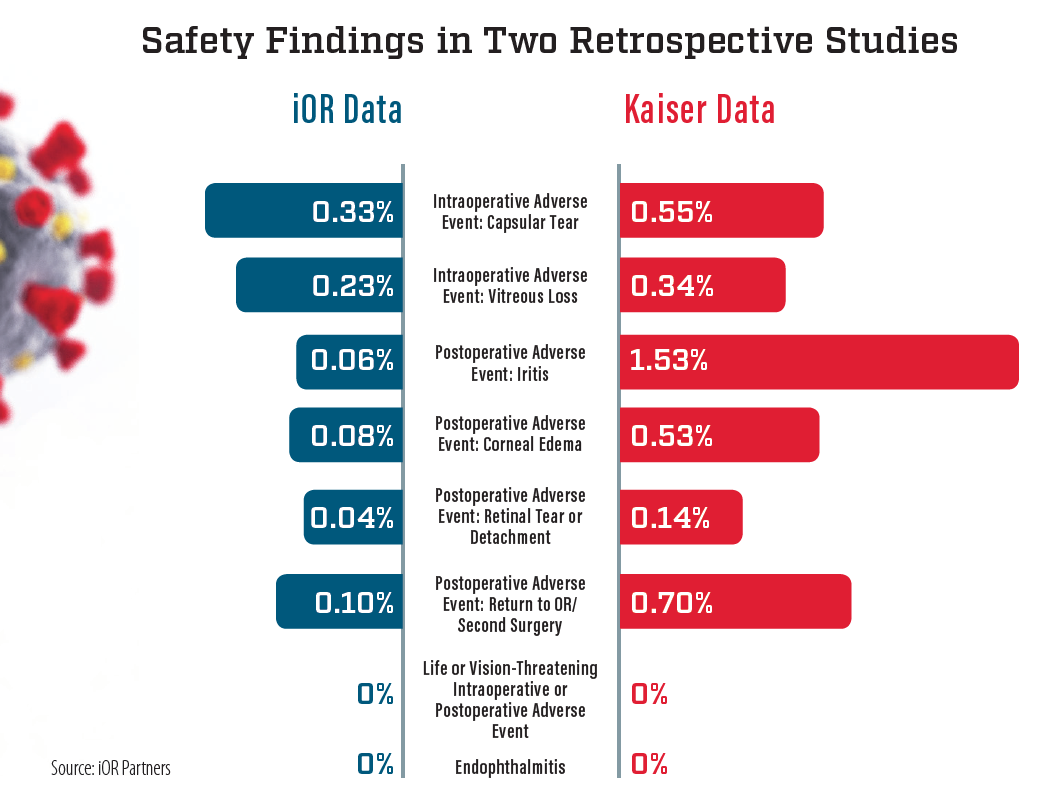
Ianchulev et al conducted a thorough safety review of office-based surgery in 2016.1 Their study included safety data on 21,501 cataract surgeries performed in Kaiser office-based surgery centers, and they concluded that safety in those centers was as good as or better than comparable data from surgery performed in ASCs. Subsequent data compiled by iOR Partners, a company specializing in development and management of office-based surgery centers, confirms the findings of that earlier study (see Safety Findings in Two Retrospective Studies).
patient comfort
For all the years I used an open-access ASC, I did not realize the anxiety it caused many patients. It turns out that most patients expect eye surgery to be performed in the surgeon’s office, and many are surprised when they are told that they must go to a third-party facility.
With office-based surgery, patients appreciate their procedure being performed in the facility to which they are accustomed. They like dealing with the same staff members they have seen during preoperative visits. This familiarity reduces anxiety and leads to a more comfortable experience.
SCHEDULING CONTROL
Office-based surgery suites provide surgeons with the ability to better control patient scheduling and flow. This can be an advantage for both surgeons and patients, as it allows the practice to offer more convenient procedure days and times. Often, procedures can be done on the same day as preoperative evaluations or testing, which is appealing for patients traveling from out of town.
The ability to schedule procedures in a familiar office at a convenient time can help to improve conversion rates for premium services, and billing for such services can also be streamlined and less cumbersome for patients and staff.
ASCs are deeply entrenched in the Medicare and insurance worlds, and administrators are often uncomfortable with cash-pay options. Such discomfort can lead to patient confusion or lost confidence in the process. All of this can be avoided with office-based procedures.
TIMELY ADVANTAGES
The myriad advantages that office-based surgery centers can offer over other types of facilities are becoming even more important amid the COVID-19 pandemic. Patients are justifiably reluctant to go to any medical facility, and they feel more comfortable in the confines of an office. Flexibility in scheduling also allows practices to implement decreased schedule density and improved social distancing, and procedures can be performed with minimal contact between patients and staff.
In multispecialty ASCs, specialized equipment, supplies, or staff for dealing with the front lines of the pandemic may be required. Eye supplies and equipment are typically not needed for other purposes, and therefore single-specialty office-based facilities may have more flexibility in opening and providing services in the current environment.
The unprecedented COVID-19 pandemic is causing surgical practices to adapt quickly. All health care providers are evaluating how to better ensure the health and safety of staff and patients, reduce patient anxiety, and provide superior surgical outcomes. For many ophthalmic surgeons, this adaptation may include transitioning to an office-based surgery center as an alternative to a hospital or ASC.
1. Ianchulev T, Litoff D, Ellinger D, Stiverson K, Packer M. Office-based cataract surgery: population health outcomes study of more than 21 000 cases in the United States. Ophthalmology. 2016;123(4):723-728.

