
CASE PRESENTATION
A 72-year-old myopic woman is referred for cataract surgery on her right eye. The patient recently lost her driver’s license because of 20/70 visual acuity in that eye, her only seeing one. She has been postponing surgery for fear of possibly losing her vision, but she cares for her grandchildren and says that she “no longer has a choice.”
Approximately 30 years ago, the patient sustained a contusion injury to her left eye associated with domestic abuse. The injury required a vitrectomy and a scleral buckling procedure for retinal detachment. She states that she saw well for a short time thereafter but has not had any formed vision in that eye for decades. She also says that she was instructed to leave her left eye alone because of a poor prognosis and a risk of complications.
On examination, the right eye is entirely normal except for a 3+ brunescent cataract. Despite myopia, the peripheral retina shows no significant pathology on ophthalmoscopy with scleral depression. There is no relative afferent or efferent pupillary defect. The left eye has light perception vision and perceives projected light in all quadrants. The patient has a variable 10–prism diopter sensory left exotropia. A slit-lamp examination shows a tan hypermature cataract. The center of the nucleus is located slightly below the pupillary center and exhibits total opacity (Figure). IOP is symmetric and in a normal range, but there is gonioscopic evidence of 2 clock hours of angle recession superiorly with 3+ pigment in the left eye only. There is no view of the fundus by indirect ophthalmoscopy. The buckle is posteriorly placed and externally well healed.
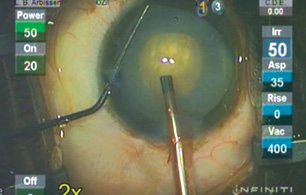
Figure. Morgagnian cataract.
How would you educate this patient and approach informed consent? On which eye would you operate? Would you plan to perform any special preoperative or intraoperative maneuvers?
—Case prepared by Lisa Brothers Arbisser, MD

JOHN C. HART JR, MD, FACS
Assuming a normal B-scan ultrasound of the patient’s left eye, I would recommend surgery on both eyes. I would operate on the left eye first. A history of domestic violence puts both eyes at risk for zonular weakness. Informed consent must therefore review the potential complications of zonular weakness as well as the issue of sensory exotropia if both eyes are treated. Optical biometry would be attempted, but immersion A-scan ultrasound would likely be required.
I would stain the anterior lens capsule of each eye with trypan blue dye under a dispersive OVD. All steps in both cases must avoid zonular stress. I would refill the anterior chamber with an OVD prior to removing coaxial instruments to avoid hypotony.
The left eye has a morgagnian cataract. After staining the anterior capsule, I would use a Kuglen hook to retract the iris and assess the eye for zonular loss. Initial entry into the anterior capsule will release liquefied lenticular material, which I would aspirate and replace with a dispersive OVD prior to completing the capsulorhexis. I would inject a dispersive OVD beneath the nuclear fragment to create space between the lens and the posterior capsule. Next, I would perform phacoemulsification of the nucleus and employ a chopping technique at the plane of the capsulorhexis. I would insert a standard capsular tension ring (CTR) and IOL.
For the right eye, I would look carefully for zonular weakness at each surgical step. Hydrodissection must be complete, allowing the nucleus to spin freely within the capsular bag. I would employ phaco chop for nuclear disassembly. I would implant a standard CTR and IOL.

RUPERT MENAPACE, MD, FEBO
I would operate on the right eye first because a successful outcome would give the patient confidence about proceeding with surgery on the left eye.
Because of the history of contusion, I would evaluate the left eye for zonular weakness by gently pressing my finger against the globe at the slit lamp under conditions of maximum pupillary dilation. Assuming that the pupil dilates well and zonular fixation is stable, I would perform phacoemulsification cataract surgery from a temporal approach. I would stain the anterior capsule with trypan blue dye (VisionBlue, Dutch Ophthalmic USA) under air and tamponade the anterior chamber with a high-viscosity OVD to flatten the apex of the lens.
After creating a small central capsulorhexis, I would perform dry aspiration of the liquefied cortex so as to avoid incurring the Argentinian flag sign. The capsulorhexis would be enlarged later. I would expect to find the shrunken nucleus floating in the capsular bag. With frequent refilling of the anterior chamber and capsular bag with Viscoat (Alcon), I would engage the nucleus with high flow and vacuum and emulsify it using burst mode and horizontal chopping. I would insert iris hooks and capsule retractors as required to relieve superiorly defective or unstable zonules. Then I would insert a CTR and a foldable IOL.
If the nucleus could not be emulsified, if a capsular complication occurred, or if zonulolysis could not be managed with CTR implantation, I would switch to a superior-access frown incision and deliver the remaining nucleus using the fishhook technique described by Hennig.1 My preference would be to fixate a Verisyse IOL (Johnson & Johnson Vision) to the iris. Scleral fixation of a three-piece IOL would be an alternative.

DENISE M. VISCO, MD, MBA
Cataract surgery on the right eye is the fastest path to restoring this patient’s visual function and allowing her to resume a normal life. The procedure should be straightforward and uncomplicated, and it should not require any special intraoperative maneuvers. I would, however, use phenylephrine and ketorolac intraocular solution 1%/0.3% (Omidria, Omeros) in the irrigating fluid to mitigate the risk of intraoperative floppy iris syndrome, intraoperative miosis, and surgical complications.2,3
Informed consent would mirror that for a routine cataract case except that it would also address the patient’s obvious concern about undergoing surgery on her better-seeing eye. I would also inform her that she has the option of surgically maximizing the visual acuity of her left eye prior to intervention in her right eye, but I would be clear that I do not recommend this approach. Instead, I would recommend addressing her left eye after restoring functional vision to her right eye. I would counsel the patient that her history of good vision after initial repair suggests the potential for vision in her left eye. That said, her exotropia puts her at risk of double vision after successful cataract surgery. Furthermore, I would expect the cataract procedure to be complex because of the identified zonular weakness.
A B-scan would show whether the retina is still attached, among other things, and I would perform this test before committing to operating on the left eye. Assuming favorable findings with a B-scan, my surgical plan would include preparations for intraoperative maneuvers to address zonular instability, such as capsular hooks, capsular tension segments, and a CTR. Softening of the mature brunescent lens with a femtosecond laser could be considered, provided that the capsulotomy’s position and size can be appropriately modified. The density of the lens may require conversion of the procedure from phacoemulsification to a modified extracapsular technique. Furthermore, if zonular stability cannot be maintained throughout the surgery, it may become necessary to sew in the IOL. Intracameral phenylephrine and ketorolac would be useful to help maintain miosis and iris tone throughout surgery.2,3 Lastly, if any portion of the lens-bag complex were to be lost in the vitreous, assistance from a retina specialist would be required.
Any procedure on the left eye would require a sophisticated armamentarium of cataract surgical skills that most surgeons—myself included—do not possess. This skill set is common, however, among surgeons who regularly handle such cases. The duty of this patient’s physician is to help her to achieve her visual goals. Guiding her through the decision-making process will involve first listening to her and then using clear language to explain her options and offer recommendations. Ultimately, the patient will decide what she wants to do, and I would respectfully facilitate her wishes as best I could.
If the reason for the nuclear displacement is the state of the lens and not the zonules, I would be more likely to recommend—and perform myself—surgery on the left eye (still after surgery on the right eye). I would also be more likely to use a femtosecond laser. The lens might be under pressure, so protective measures against the Argentinian flag sign would be necessary. In that scenario, in my hands, use of a laser has been more successful than needle decompression with a manual capsulotomy.

WHAT I DID: LISA BROTHERS ARBISSER, MD
After a thorough discussion of the likelihood of achieving useful vision in the left eye and despite a guarded prognosis for driving vision, the patient opted to undergo cataract surgery on the left eye first. Surgery was scheduled for 2 weeks later. She understood that she might have double vision postoperatively that would likely be transient but could require further surgery. All of the usual risks were discussed and emphasized.
Because the patient could not fixate reliably on the muscle light, I opted for peribulbar anesthesia. B-scan ultrasonography showed an attached retina with a high buckle. I used an immersion A-scan and the patient’s refractive history and biometric parameters for the fellow eye to determine IOL power. She chose a target of emmetropia (with the same plan for the fellow eye in time) because she was accustomed to wearing glasses. The amount of astigmatism was trivial.
Customization of her surgery included a bolus dose of intravenous mannitol of 0.25 g/kg 20 minutes before the incision, a soft-shell OVD technique employing Healon5 (Johnson & Johnson Vision) and Viscoat, trypan blue dye, and an oral 500-mg acetazolamide sequel upon discharge. Supplemental tools were available in case conversion to extracapsular surgery or performance of a one-port pars plana vitrectomy became necessary or zonular pathology required management. I also, of course, had a backup lens available in addition to the one-piece acrylic IOL.
I stained the capsule under the soft-shell OVDs with trypan blue dye and replaced the Healon5 to flatten the anterior curve of the intumescent lens dome. Because the nucleus was free-floating, I could have aspirated milky cortex with a syringe needle after puncturing the anterior capsule. This is not my usual procedure for intumescent lenses because intralenticular pressure loculated behind the nucleus can push a large nucleus forward once the anterior pressure is relieved, causing a ball-valve effect. Subsequent decompression can still result in the Argentinian flag sign. Instead, I created a small, tight flap with a cystotome and then used Viscoat to push away visually obstructing lens milk sequentially as it presented. This technique allowed me to make a conservative curvilinear capsulorhexis safely because the chamber never became shallow. With this technique, I can spiral out or enlarge the capsulorhexis as I gain control, initially and/or later in the procedure. I have never experienced a tear with this approach.
I performed minimal hydrodissection just sufficient to decompress the bag and confirm that the nucleus was mobile. I entered the OVD-controlled anterior chamber with the phaco tip on footpedal position zero and lifted the iris off the anterior capsule with a chopper before initiating irrigation to prevent retropulsion of the iris and reverse pupillary block. It is important to establish flow in an OVD-filled environment before initiating ultrasound to prevent wound burn.
My usual technique of circumferential disassembly with cross-action vertical chopping for brunescent lenses proved somewhat more difficult than usual due to the mobility of the nucleus.4 This technique has the advantage of keeping all ultrasound at or below the iris plane. It requires tight incisions, including a small paracentesis, to avoid leakage of balanced saline solution and migration of fragments into the paracentesis. I use a Rosen splitter as my chopper because it is not sharp and works well for all lenses regardless of density. I prefer burst mode for nuclear disassembly and set it according to density; 80% to 90% ultrasound was required for this leathery, tan lens. This strategy provides me with excellent control without clogging because the linear footpedal position controls burst interval rather than power.
I impaled the nucleus and then performed superficial vertical chops, not intended to progress through the leathery posterior plate but to give me access to the mature endonucleus. I sequentially debulked the lens from the inside out and actively fed material to the tip. I left the nucleofied epinuclear shell in the bag until last to protect the posterior capsule until the final dense fragments had been removed. Because of the liquid nature of the cortex, I reinstilled a dispersive OVD more than once. Toward the end of the case, I sandwiched the remaining epinuclear fragments in an OVD to hold back the posterior capsule and maintain control.
I generally avoid a supracapsular procedure, even for an eye with a morgagnian lens, and keep everything in its physiologic position as much as possible. In my experience, the cornea is clear on postoperative day 1, even in eyes that had the densest of nuclei. Despite the laboriousness of phacoemulsification in this case, total cumulative dispersed energy was only 31.29 seconds because there was no sculpting and I applied ultrasound energy only to gain purchase for mechanical forces with the chopper and to assist with aspiration as needed. There were no zonular issues and no formed cortex, and it was easy to polish the capsule clear. I implanted a one-piece lens without difficulty and enlarged the capsulorhexis to fit the IOL. The main clear corneal incision was watertight without a stitch, but a suture was required for the paracentesis, which had been stretched slightly. I used intracameral moxifloxacin, off-label, as has been my routine since 2007.
To everyone’s surprise and delight, UCVA was 20/20 on postoperative day 1. I gave the patient readers. She now favored the visual acuity of her left eye to that of her right. Subsequently, she underwent uneventful cataract surgery on her second eye under topical anesthesia. After surgery, she experienced only 1 day of inconstant diplopia. She was able to drive herself to and from her postoperative appointments and drive her grandchildren to school.
1. Hennig A. Nucleus management with fishhook. Indian J Ophthalmol. 2009;57(1):35-37.
2. Silverstein SM, Rana VK, Stephens R, et al. Effect of phenylephrine 1.0%-ketorolac 0.3% injection on tamsulosin-associated intraoperative floppy-iris syndrome. J Cataract Refract Surg. 2018;44(9):1103-1108.
3. Rosenberg ED, Nattis AS, Alevi D, et al. Visual outcomes, efficacy, and surgical complications associated with intracameral phenylephrine 1.0%/ ketorolac 0.3% administered during cataract surgery. Clin Ophthalmol. 2017;12:21-28.
4. Arbisser LB. Advanced phaco techniques for brunescent nuclei: cross-action chop circumferential disassembly. In: Chang DF, ed. Phaco Chop and Advanced Phaco Techniques. 2nd ed. Thorofare, NJ: Slack; 2013: 221-229.

