We encounter many cataract surgery patients with pupils that dilate insufficiently. The typical cataract is about 9 to 10 mm in diameter, and it has to come out of the eye through the capsulorhexis and the pupil during cataract surgery. We break the cataract nucleus into pieces to aid in this process, but a small pupil makes the surgery significantly more challenging. If we can achieve about a 5-mm pupil and a 5-mm capsulorhexis, the surgery will be much smoother, will be safer for the patient, and will be less stressful for us.
There are multiple options available to achieve pupil expansion and facilitate successful cataract surgery. Surgeons can use a stepwise approach in eyes with insufficient dilation, starting with pharmacologic agents, progressing to viscomydriasis, then stretching the pupil, and, finally, using a pupil expansion device. This article reviews some of the options available to expand a small pupil and ease the course of cataract surgery.
PHARMACOLOGIC AGENTS
Standard topical pharmacologic dilation usually includes some combination of agents such as phenylephrine 2.5%, tropicamide 1%, or cyclopentolate 1%. The effect can be augmented by using higher concentrations, such as phenylephrine 10%. These agents should be given plenty of time to work, with surgery performed about 30 minutes after instillation.
Three Tips for Cataract Surgery in Eyes With Small Pupils
Without using iris hooks or expanders.
• Tip No. 1: Stretch the pupil and viscodilate
Use two choppers or other instruments to engage the pupillary margin at two points 180º apart. Then stretch the pupil all the way to the angle of the eye. Use OVD to further expand the pupil and keep it that way to make plenty of room for the capsulorhexis.
• Tip No. 2: Make the capsulorhexis larger than the pupil
You do not need to directly visualize the edge of the capsulorhexis to know where it is. If you can get the pupil up to 4 mm in diameter with stretching and viscomydriasis, then you can make a capsulorhexis 5.0 or 5.5 mm in diameter. Have faith and make the capsulorhexis larger than the pupil.
• Tip No. 3: Bring the nucleus out of the capsular bag
Using careful, slow hydrodissection, bring the cataract nucleus partially out of the capsular bag and into the iris plane. The iris will now help to hold the nucleus in place as you chop it and use the phaco probe to emulsify it.
In addition, studies have shown that preoperative application of a topical nonsteroidal antiinflammatory drug can help maintain mydriasis during surgery. There are also commercially available combinations of some of these pharmacologic agents that can be used for constant infusion during phacoemulsification.
Individual aliquots of medications such as preservative-free phenylephrine and lidocaine can also be administered directly into the anterior chamber to aid in pupillary dilation. Some surgeons even use dilutions of epinephrine (eg, 1:5,000), with balanced salt solution as the diluent.
VISCOMYDRIASIS
In viscomydriasis, a technique described by Robert H. Osher, MD, an OVD is used to push the iris outward and expand the pupil. This can be done to aid in capsulorhexis creation, although the effect is short-lived. As soon as the OVD is removed from the eye, the pupil starts to come down.
Performing cataract surgery in an eye with a midsized pupil of about 3 or 4 mm diameter does not typically require the use of iris hooks or iris expansion devices. The surgeon can simply instill anesthetic and mydriatric agents and then use the OVD to perform viscomydriasis, which will provide an additional 1 or 2 mm of pupil expansion.
In viscomydriasis, the OVD is injected at the pupillary margin to push the iris toward the angle of the eye. You can make the capsulorhexis larger than the pupil without directly seeing the edge by carefully going under the iris. It’s in your mind: You know where the capsulorhexis should be, and you just have to have faith and go for it. You will be able to create a great capsulorhexis without seeing the edge. When this step is complete, the lens nucleus can be prolapsed out of the capsular bag and held in position by the iris.
If the pupil does not dilate sufficiently with the steps described so far, you can proceed to pupil stretching, using iris hooks, or inserting a pupil-expansion ring. Any of these processes can create a maximum pupillary opening of about the same circumference or perimeter, which means that the amount of iatrogenic trauma to the pupillary sphincter is similar with each (Figure 1).
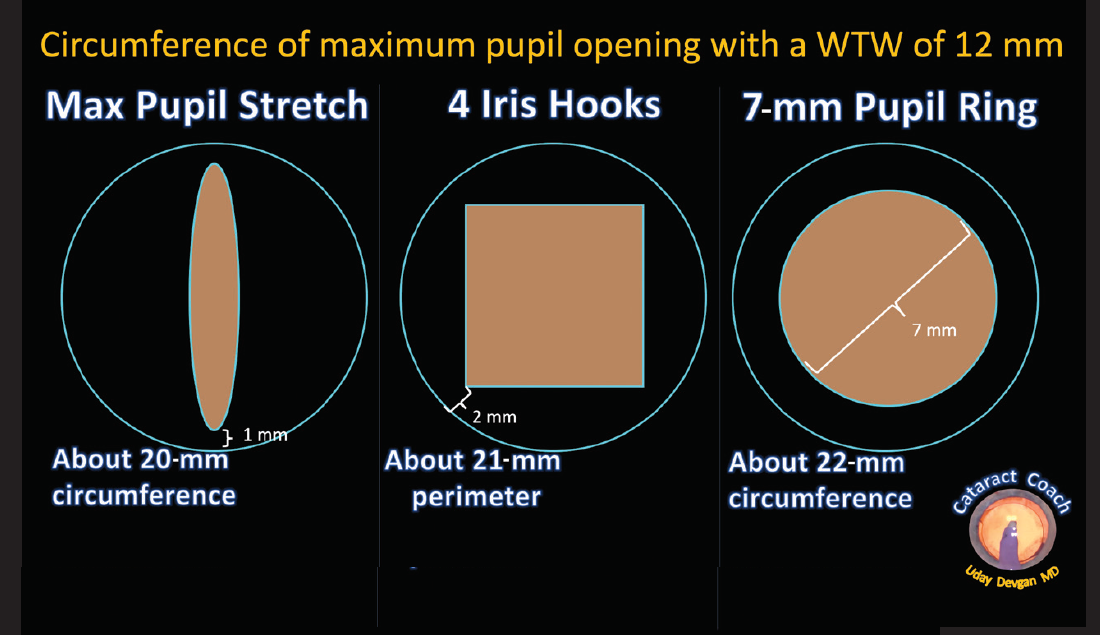
Figure 1. Whether pupil stretching, iris hooks, or expansion rings are used, the circumference of the maximum pupil opening will be about the same. Abbreviation: WTW, white-to-white distance
PUPIL STRETCHING
Stretching the pupil mechanically causes microtears of the sphincter and allows greater dilation. There are specially designed instruments for this purpose, such as two-, three-, and four-pronged pupil dilators, but there are also simpler options. For example, two choppers or similar instruments can be used to perform the stretching.
Two instruments, one in each hand, are used to securely hold the pupillary margin at opposite sides. The instruments are then moved apart, toward the angle of the eye on either side. This can be repeated after shifting the instruments 90º to ensure a sufficient stretch. Then more OVD can be used to hold back the iris, and you can proceed with the remainder of the case.
As noted, you don’t need special instruments to do this. With two instruments such as choppers, hooks, or manipulators, the iris can be held and stretched quite effectively. You can even make use of instruments already on your surgical tray, using the capsulorhexis forceps to grab one part of the iris while the chopper engages the opposite side (Figure 2).
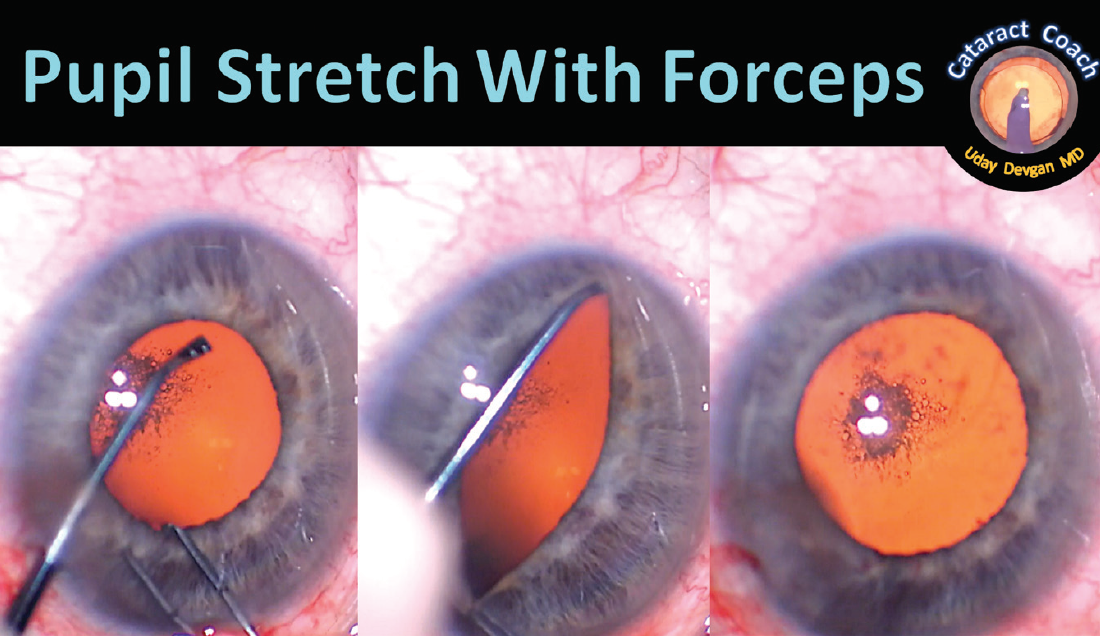
Figure 2. With a chopper in the left hand and capsulorhexis forceps in the right, the iris stroma is gently grasped at the pupil margin and engaged at the opposite edge, and then the stretch maneuver is performed.
HOOKS AND RINGS
If stretching fails, pupil expansion devices such as iris hooks and pupil expander rings are useful in eyes with miotic pupils. These devices must be inserted as gently and atraumatically as possible to avoid doing damage to the iris. Too much iris manipulation can also lead to increased levels of postoperative inflammation and longer recovery. The amount of pupil sphincter trauma will be similar with these devices as with manual stretching (Figure 3).
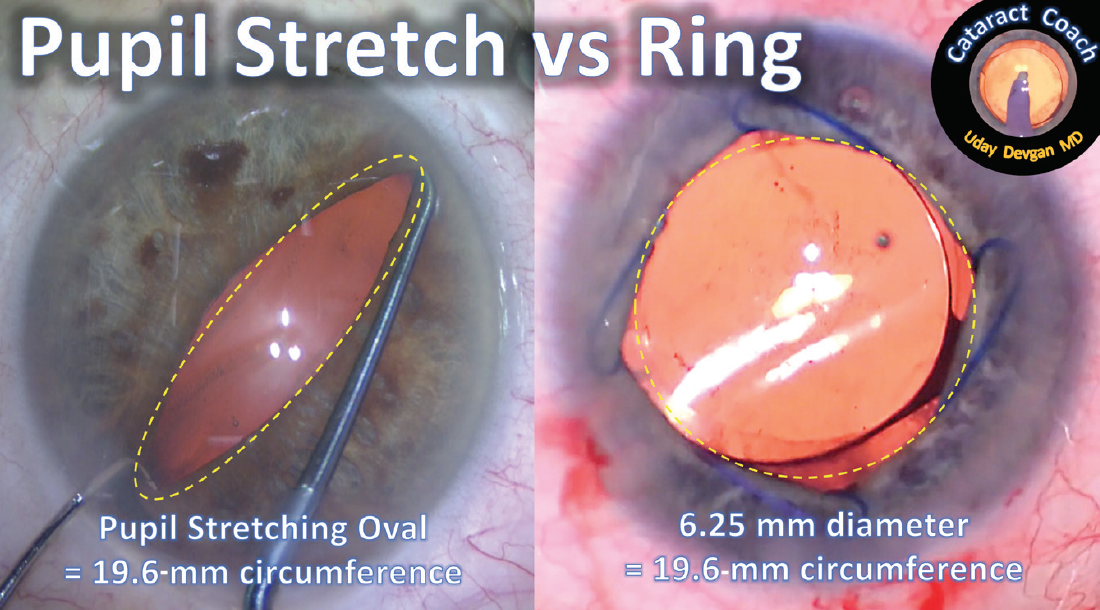
Figure 3. The pupil expander was inserted in this eye with three of the four fixation points secured using only the injector.
A few tips and tricks can make placement of a pupil expansion ring easier. Using OVD, tent up the iris in the four spots where the scrolls or coils of the ring will engage the iris. These dollops of OVD will lift the iris above the anterior lens capsule and facilitate ring placement. In the case shown in Figure 4, I was able to engage three of the four scrolls with the iris edge using just the inserter device alone.
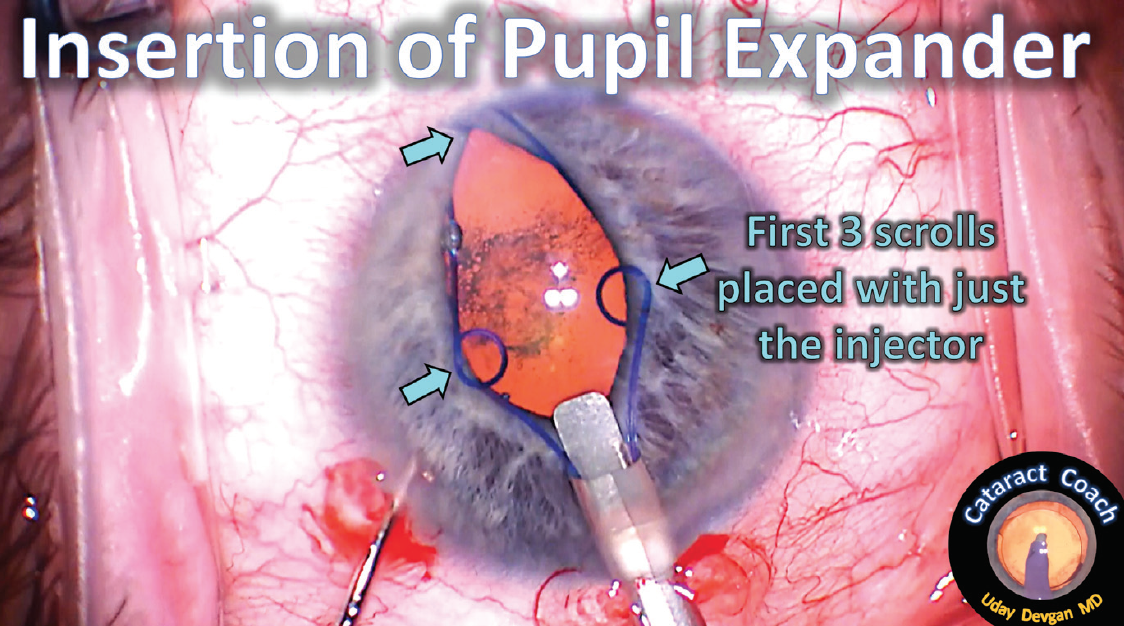
Figure 4. Both pupil stretching and implantation of a 6.25-mm pupil expansion ring will produce the same circumference and thus a similar degree of iris sphincter muscle trauma.
After the four scrolls are placed, the ring can be centered in the eye using any instrument. Just after ring placement, the pupil center may be displaced, but the ring can easily be shifted and the pupil centered again. To remove the device, all four scrolls are unhooked, and then the original injector is used to catch the ring at any point and retract it into the shaft of the injector. The ring may become bent or twisted, but because this is a single-use device, it will be discarded anyway.
Many devices are available for this purpose, including disposable and reusable iris hooks and pupil expansion rings from different manufacturers. One interesting device that may be available soon is the B-Hex Pupil Expander (Med Invent Devices) developed by Suven Bhattacharjee, MD. This device goes through a sub–1-mm incision and has a low-profile design that creates a hexagonal pupil during surgery.1
How does pupil stretching compare with use of a pupil expansion device? The anatomic results are similar. I was able to make a contralateral eye comparison in a recent patient. His right eye received an expansion ring (Figure 4) during cataract surgery, and in his left eye, I used pupil stretching with forceps and a chopper (Figure 2). At the end of the case, the structural and anatomic results for the two pupils were essentially the same (Figure 5).
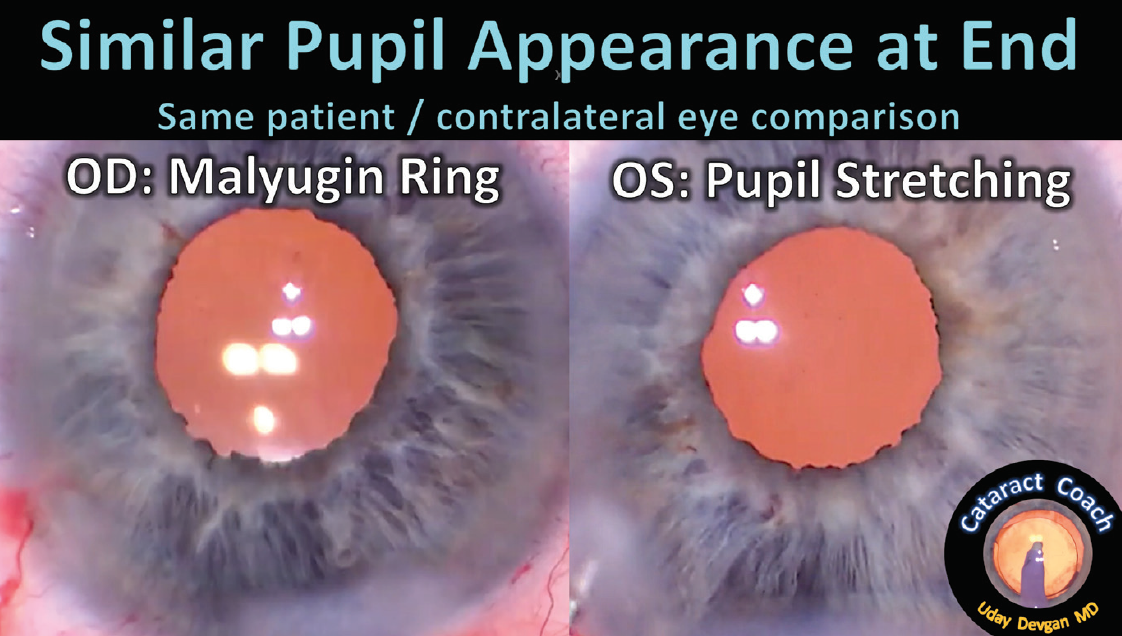
Figure 5. Whether a pupil expansion ring or pupil stretching technique is used, the pupil appearance at the end of the surgery is similar, with multiple microtears in the iris sphincter.
Rarely, one of these processes can cause a cosmetic defect such as corectopia, although this will have minimal, if any, effect on visual outcomes.
ONE FINAL TIP
After IOL insertion but before removal of the OVD, the chopper can be used to tent up the iris around 360º to allow you to check whether any residual cortex or nuclear chips remain. During this maneuver, you can also verify that the IOL optic is behind the capsulorhexis and in proper position (Figure 6).
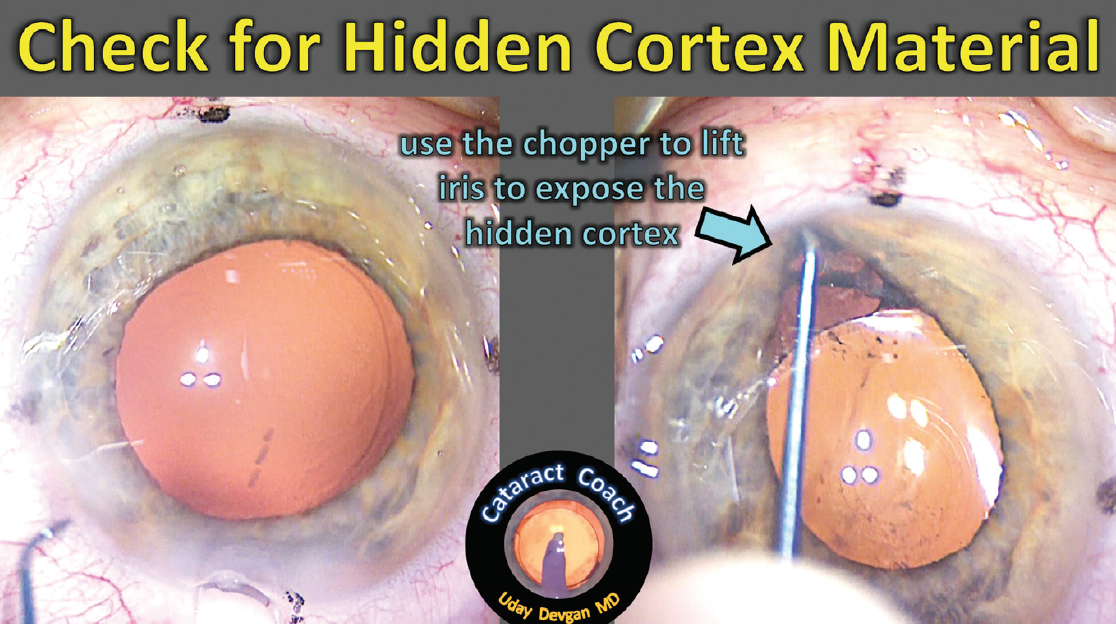
Figure 6. The chopper is used at the end of the case to lift the iris in all quadrants to make sure that no retained lens material, such as cortex as shown here, is left behind.
The next time you encounter a small pupil in a patient undergoing cataract surgery, try this stepwise approach: pharmacologic agents first, then viscomydriasis, moving on to pupil stretching, and finally the use of expansion devices. Videos and further reading on this topic may be found at www.CataractCoach.com.
1. Bhattacharjee S. B-Hex Pupil Expander: pupil expansion redefined. Indian J Ophthalmol. 2017;65(12):1407-1410.