



The Trulign Toric (Bausch + Lomb) posterior chamber accommodating IOL was launched in 2013, with available spherical powers ranging from +17.00 to +25.00 D. Recently, the spherical power range was extended down to +10.00 D, allowing use of the lens in more myopic patients. These individuals tend to have greater axial lengths, deeper anterior chambers, and larger capsular bags, all of which can affect an IOL’s stability.
The expanded range of the Trulign provides an alternative to the one-piece acrylic toric IOLs for patients with high myopia and astigmatism who desire both distance and intermediate vision in addition to astigmatic correction.
THE INVESTIGATION
I had a substantial number of motivated, highly myopic patients with symmetrical astigmatism who were interested in achieving unaided intermediate vision to see their computers and e-tablets in my practice. The extended range of spherical powers in the Trulign family allowed me to provide them with this option.
Out of concern over the IOL’s rotational stability in high myopes, I decided to track outcomes for patients who received these low-diopter IOLs. I collected 1-month post cataract surgery refractive and visual acuity data for a series of 21 consecutive eyes implanted with Trulign Toric IOLs in powers from +10.00 to +16.00 D. The data included all patients who received the lens within this power range. I performed the surgery on all of the eyes with my typical supracapsular phaco technique. No intraoperative aberrometry was performed in any of these cases, because I did not have access to the ORA System (Alcon) at that time.
MEASURES OF INTEREST
Measures of interest to me were the residual manifest refraction, both the spherical equivalent and the residual cylinder, and the UCVA achieved at distance, intermediate (26 inches), and near (16 inches). With people’s ever-increasing use of handheld devices, intermediate vision is becoming more important to patients.
Preoperative UCVA in this group of patients ranged from 20/50 to count fingers vision. Average axial length in these eyes was 26 mm, with a minimum of 24.33 mm and a maximum of 27.42 mm. All of these patients had symmetrical astigmatism greater than or equal to 1.00 D.
I implanted IOLs with spherical powers from +10.00 to +16.00 D and a variety of cylindrical powers. Specifically, 19% of eyes received the 1.25 D cylinder lens, 52% the 2.00 D cylinder lens, and 29% the 2.75 D cylinder lens. The cylindrical powers listed here are measured at the IOL plane. I used the Holladay 2 formula with and without the Wang/Koch adjustment to calculate my IOL powers.
RESULTS
Postoperative results were excellent. The mean spherical equivalent refraction was -0.42 ±0.39 D, with a range of +0.38 to -1.38 D (two eyes were targeted for intermediate vision). More than 85% of eyes (17/21) were within 0.50 D of their targeted refraction. More than half of this group (12/21, 57%) had zero manifest refractive cylinder postoperatively, and 95% (20/21) had 0.50 D or less; these results are better than those reported in the clinical trial submitted to the FDA for the original Trulign Toric IOL’s approval. I observed no cases of Z syndrome, and no laser touchups were required for any patient.
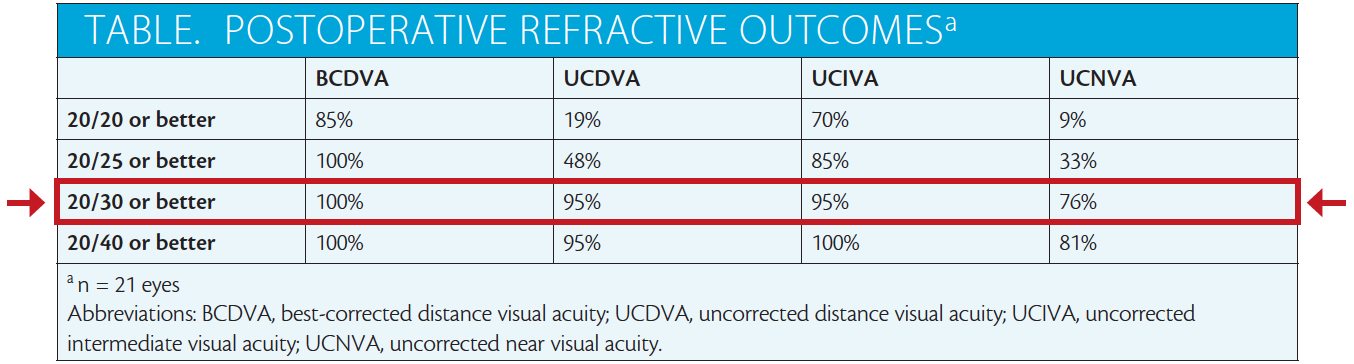
The table contains the summary data for distance BCVA and distance UCVA as well as intermediate UCVA and near UCVA. Patients achieved very good distance and intermediate vision, with functional near vision, as is typical of the Trulign Toric lens.1
WOUND CLOSURE
I believe one of the keys to the successful results in these long eyes is a secure, watertight wound. It is essential to ensure rotational stability of the IOL in the bag at exactly the axis where it was placed. For many years, I used a 10–O Vicryl suture (Ethicon) for wound closure in eyes that received an accommodating IOL. My new approach involves using ReSure Sealant (Ocular Therapeutix), a hydrogel ocular sealant indicated for the intraoperative management of clear corneal incisions. I find the sealant is easy to apply by painting the mixture over the sponge-dried main and sideport corneal incisions.
Some surgeons have concerns about the rotational stability of toric IOLs, especially in high myopes, where the capsular bag can be large and the implant may have a higher likelihood of rotation. An unstable anterior chamber from a microleak can increase the risk of such a rotation. Using the sealant, I am confident that the anterior chamber will remain stable after surgery. My postoperative outcomes show that the low-powered Trulign Toric IOL provided excellent distance and intermediate vision and adequate near vision with no rotational issues.
Watch it Now
Cynthia Matossian, MD, demonstrates her technique for the Trulign Toric IOL’s insertion and the ReSure sealant.


CONCLUSION
In my hands, the low-diopter Trulign Toric IOL has effectively reduced refractive cylinder and improved distance and intermediate vision in myopic patients. I feel that use of the ReSure Sealant contributes to my success in these cases. I use it in all of my patients receiving the Crystalens (Bausch + Lomb) or Trulign Toric lens. n
1. Trulign Toric IOL [package insert]. Abbott Park, IL: Abbott; 2016.

