





The treatment of corneal endothelial decompensation is challenging. The most common form of corneal endothelial disease, Fuchs endothelial corneal dystrophy (FECD), affects approximately 4% of the US population who are over 40 years of age. Without intervention, FECD results in vision loss, pain, and potentially blindness.1
Currently, the gold standard for the treatment of visually significant corneal endothelial dystrophy is partial-thickness corneal transplantation—either Descemet stripping or Descemet membrane endothelial keratoplasty. Three emerging techniques hold promise for the treatment of corneal endothelial disease without corneal transplantation.
RIPASUDIL
Rho kinase (ROCK) inhibitors have attracted considerable interest in regenerative medicine to heal the corneal endothelium. This class of medication facilitates the proliferation of corneal endothelial cells by promoting the transition from the G1 phase to the S phase of the cell cycle. ROCK inhibitors can also inhibit actin-myosin contraction, thereby promoting cell migration and adhesion.
A critical review highlighted the current evidence supporting the use of the ROCK inhibitor ripasudil to treat corneal endothelial disease.2 Research on the drug’s clinical usefulness in this field has focused primarily on its ability to enhance the regeneration of Descemet membrane after descemetorhexis without endothelial keratoplasty, known as Descemet stripping only (DSO), surgery in patients with FECD. This could obviate the need for corneal transplantation and its inherent risks, such as graft rejection, detachment, and corticosteroid use. Studies have indicated that descemetorhexis without endothelial keratoplasty/DSO with ripasudil achieves similar outcomes but with fewer adverse events compared to traditional Descemet membrane endothelial keratoplasty in select patients.2 There have also been isolated case reports of the successful use of ripasudil for managing pseudophakic bullous keratopathy without surgery.3
CELL THERAPY
Human cultured endothelial cells with ROCK inhibitor. Aurion Biotech is developing the use of cultured donor corneal endothelial cells (CECs) with the ROCK inhibitor Y-27632 injected into the anterior chamber.
A nonrandomized, single-group study enrolled patients with pseudophakic bullous keratopathy who had no detectable CECs and a corneal thickness that was greater than 630 μm.4 Purified CECs were cultured in vitro from the corneas of deceased donors. Following removal of endothelial cells, the cultured CECs supplemented with Y-27632 were injected into the anterior chamber of 11 eyes.
Twenty-four weeks after the procedure, the primary outcome (CEC density > 500 cells/mm2) had been achieved in all 11 eyes, and the mean CEC density was 1,924 cells/mm2. The secondary outcome (posttreatment corneal thickness < 630 μm) was achieved in 10 eyes, and the mean corneal pachymetry reading was 549 μm. Mean logMAR BCVA improved from an initial mean of 0.88 to 0.04, which roughly translates to a change from 20/150 to 20/20 in Snellen values. A sustained normalization of corneal endothelial function was confirmed 5 years postoperatively for 10 patients.5
In addition to reducing or avoiding the need for transplantation surgery, this method allows multiple patients to be treated with tissue from a single donor cornea.
Magnetic cell therapy. Emmecell is investigating the healing of corneal endothelial decompensation with cultured, magnetic, human CECs. The company seeks to address the challenges of cell therapy—delivery, retention, and integration—with its magnetic cell technology platform. After intracameral injection, magnetic CECs are localized to the endothelium with an external magnetic patch.
Preclinical studies in rabbit models of endothelial dysfunction demonstrated safety and efficacy when 0.2 or 0.5 x 106 cells were injected into the anterior chamber.6 Magnetic CEC delivery avoided IOP elevation and prevented the deposition of cells in the trabecular meshwork or iris. After a 6-week follow-up, the structural integrity of the endothelium and Descemet membrane was confirmed by histologic examination. The expression of human endothelial cell markers in the rabbit cornea and normal corneal anatomy indicated that the CECs had organized appropriately during the healing period.
A prospective, multicenter, phase 1 study is underway in the United States. Twenty-one patients have been treated in an open-label, dose-escalation protocol that has tested four different doses in two cohorts receiving cell injection with or without endothelial brushing or Descemet stripping.7 The four doses tested (0.05, 0.15, 0.50, and 1.0 x 106 cells) were safe, and efficacy appeared to be dose-dependent. To eliminate data analysis bias and identify the therapeutic dose, a randomized, double-masked trial is currently enrolling an additional 21 patients at nine clinical sites across the country.
FIBROBLAST GROWTH FACTOR 1 ANALOG
Trefoil Therapeutics has been exploring the use of fibroblast growth factors (FGFs) in regenerative medicine. FGFs are endogenous stimulators of CEC migration, proliferation, and wound healing in vitro. Naturally occurring FGF1, however, has proven too unreliable and unstable to be utilized clinically. TTHX1114 is an FGF1 analog modified to increase the molecule’s stability and bioavailability.
An in vitro study conducted by Trefoil Therapeutics found that administering TTHX1114 accelerated healing and regeneration of the CEC layer (Figure 1).8 Ten pairs of ex vivo healthy corneas underwent DSO. The left cornea (control) was treated with 0.8% fetal bovine serum medium. The right cornea (treatment group) was treated with the same medium and 10 ng/mL of TTHX1114. Eyes were then monitored for 14 days.
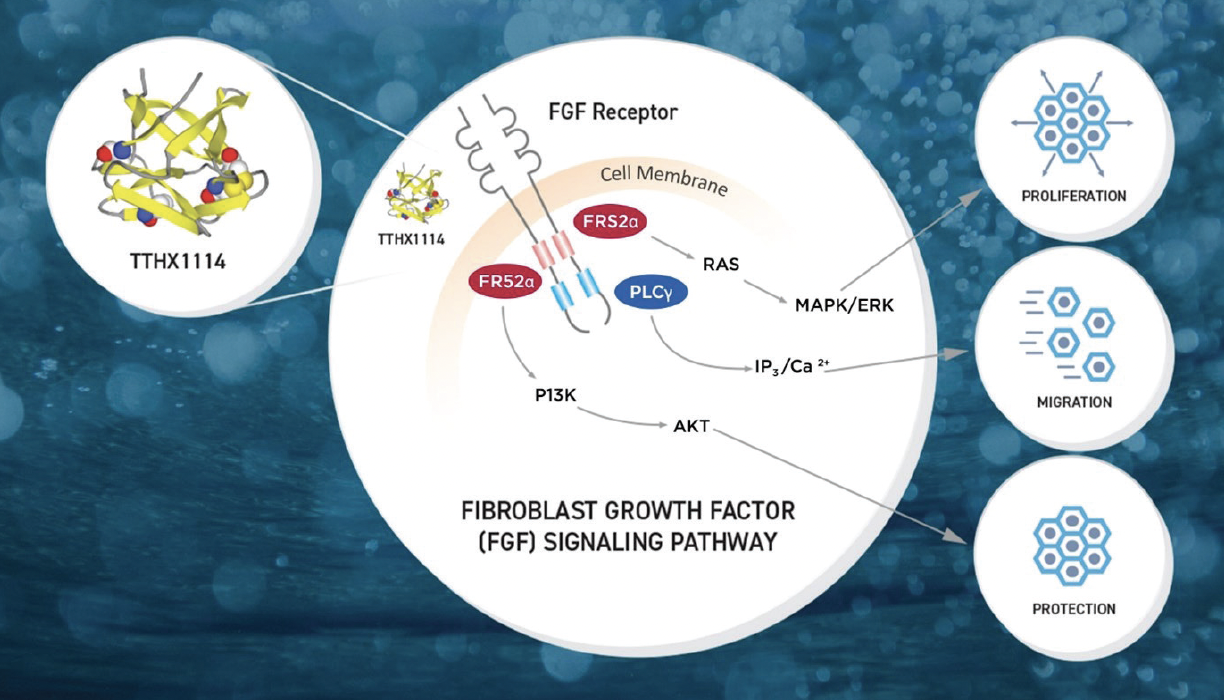
Figure 1. The mechanism of action of TTHX1114 and its interaction with the FGF receptor to induce the signaling cascade.
Figures courtesy of Trefoil Therapeutics
Healing was observed in 32% ±11% and 81% ±15% (P < .001) of the control and TTHX1114-treated corneas, respectively. In both groups, healing proceeded from the periphery to the center of the cornea. The protocol was subsequently repeated with dystrophic corneas and demonstrated similar rates of healing. At 14 days, 38% ±23% and 91% ±18% (P < .001) healing was observed in the control and TTHX1114-treated corneas, respectively. CEC density was 1,864 mm2 in the dystrophic corneas versus 2,731 mm2 in the healthy group. The treatment of ex vivo corneas with TTHX1114 dramatically accelerated the healing of the CEC layer in both healthy and diseased corneas (Figure 2).
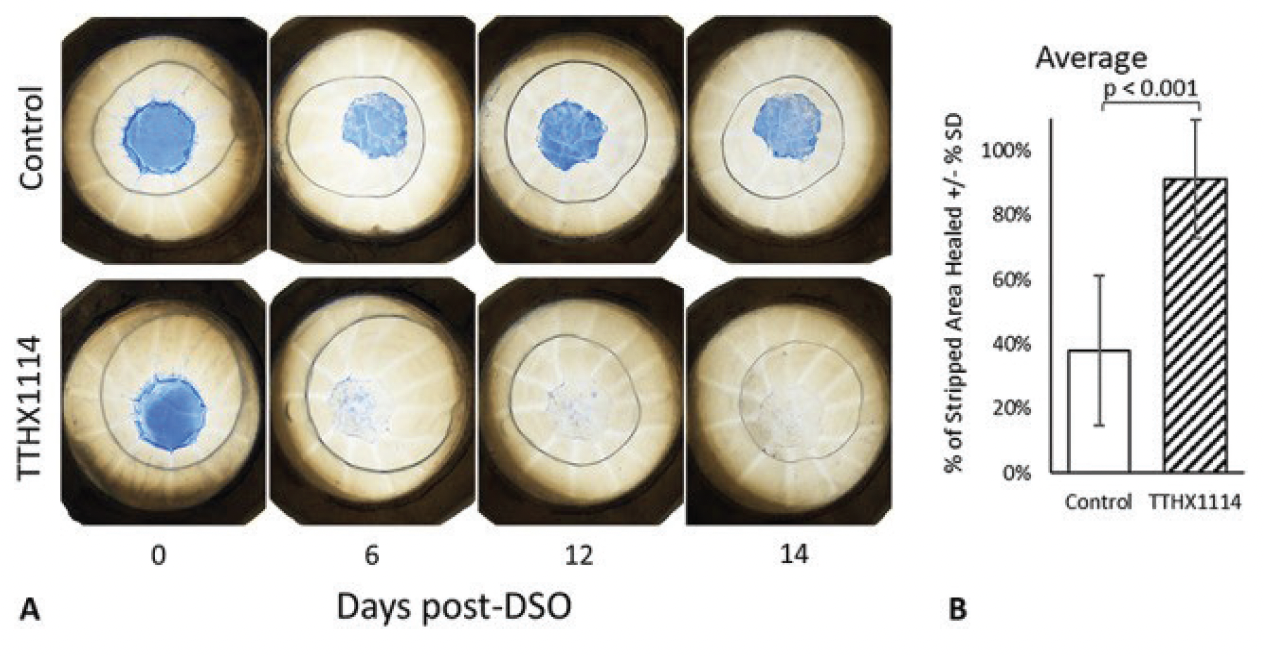
Figure 2. Healing of the corneal endothelial layer in eyes with corneal dystrophy during the 14 days following DSO. The bar graph at right compares the percentage of area healed in control and TTHX1114-treated corneas.
The company recently presented clinical data from the phase 2 STORM study that showed TTHX1114 accelerated the rate of visual recovery after DSO.9 The investigators concluded that the drug increased visual improvement and clearing of corneal edema after DSO surgery. The study has not yet undergone peer review.
CONCLUSION
The use of regenerative medicine for the treatment of corneal dystrophies shows promise. If the therapies discussed here gain FDA approval, they have the potential to revolutionize the way ophthalmologists treat corneal endothelial disease. Whether used individually or in combination, the therapies could mitigate or eliminate the need for corneal transplantation to treat FECD and other endothelial diseases.
1. Dhaliwal DK, Chirikov V, Schmier J, Rege S, Newton S. Cost burden of endothelial keratoplasty in Fuchs endothelial dystrophy: real-world analysis of a commercially insured US population (2014-2019). Clin Ophthalmol. 2022;16:1055-1067.
2. Karri R, Chong EW. ROCK inhibitors in ophthalmology: a critical review of the existing clinical evidence. Clin Exp Ophthalmol. 2023;51(5):472-483.
3. Yoshida M, Yokokura S, Hariya T, Kobayashi W, Hashimoto K, Nakazawa T. Ripasudil eyedrops ameliorated bullous keratopathy complicated with cytomegalovirus corneal endotheliitis: a case report. Ocul Immunol Inflamm. 2023;31(1):207-210.
4. Kinoshita S, Koizumi N, Ueno M, et al. Injection of cultured cells with a ROCK Inhibitor for bullous keratopathy. N Engl J Med. 2018;378(11):995-1003.
5. Numa K, Imai K, Ueno M, et al. Five-year follow-up of first 11 patients undergoing injection of cultured corneal endothelial cells for corneal endothelial failure. Ophthalmology. 2021;128(4):504-514.
6. Xia X, Atkins M, Dalal R, et al. Magnetic human corneal endothelial cell transplant: delivery, retention, and short-term efficacy. Invest Ophthalmol Vis Sci. 2019 ;60(7):2438-2448.
7. Study of safety and tolerability of EO2002 in the treatment of corneal edema. US National Library of Medicine. Updated July 18, 2023. Accessed September 22, 2023. https://classic.clinicaltrials.gov/ct2/show/NCT04894110
8. Pizzuto S, Duffey G, Weant J, Eveleth D. Acceleration of regeneration of the corneal endothelial layer after Descemet stripping induced by the engineered FGF TTHX1114 in human corneas in organ culture. Cornea. 2023;42(2):232-242.
9. Baartman BED, Greenwood M, Swan R, Berdahl J, Tremblay T, Pleil A. A phase 2 study of an engineered fibroblast growth factor (FGF) to accelerate visual recovery after Descemet stripping only (DSO). Paper presented at: ASCRS Annual Meeting; May 8 2023; San Diego.

