



The anterior capsulotomy is arguably the most crucial step of cataract surgery, whether an extracapsular, a manual small-incision, or phaco technique is used. Like the cataract surgery procedure itself, the capsulotomy has evolved. The earliest technique was to puncture and tear the anterior capsule with a Von Graefe cataract knife while creating an 180º ab interno dissection. With the evolution to ab externo techniques, a toothed forceps was used to grasp and rip the anterior capsule.1 Other once-popular approaches include a Christmas tree approach with a dull cystotome to peel and tear anterior capsular cortex into a triangular shape.2 Later, a can-opener capsulotomy with a cystotome was developed to connect multiple radial perforations of the anterior capsule and create a large opening.1 IOL decentrations and capsular fibrotic opacifications were common sequelae.
A simple technique using multiple tiny tears made circumferentially instead of radially was later introduced. The capsulotomy punctures were made on the intact anterior capsule in front of the tear and joined by a tear about 0.5 to 1 mm in diameter. The technique avoided multiple free capsular flaps, maintained the circular capsulotomy configuration, and allowed the IOL to be placed inside the capsular bag. The goal was to make a large rhexis. In the mid-1980s, Gimbel and Neuhann independently developed and introduced two similar techniques,3 which are now known as the continuous curvilinear capsulorhexis (CCC). The main advantage of the CCC, when executed correctly, is that it has a strong rim, does not have any flaps, and reduces the risk of errant tears and radial extensions. If there is a breach in the continuity of the CCC, the lens capsule can tear and run off, sometimes to the equator and beyond. If the CCC is not perfect, care must be taken to avoid aggressive extrinsic forces and pressure fluctuations.
I have developed a maneuver I call the bag handle capsulorhexis, which I believe reduces the risk of a tear-out, especially in young eyes with weak zonules. In this setting, the capsulorhexis can be difficult to complete because of a lack of support and zonular countertraction.
THE TECHNIQUE
A video demonstration of the bag handle technique can be viewed below. In the video, the technique is used in the eye of a young woman with bilateral microspherophakia, lenticular high myopic astigmatism, and a shallow anterior chamber. The patient experienced painful recurrent IOP spikes due to repeat pupillary block that were relieved with an Nd:YAG iridotomy.
Step No. 1. Under proparacaine topical anesthesia, a 2.8-mm tunnel incision is made in the peripheral cornea from the anterior sclera with a knife followed by the creation of two sideport incisions with a 21-gauge microvitreoretinal blade to facilitate capsular access and IOL enclavation (Figure 1).
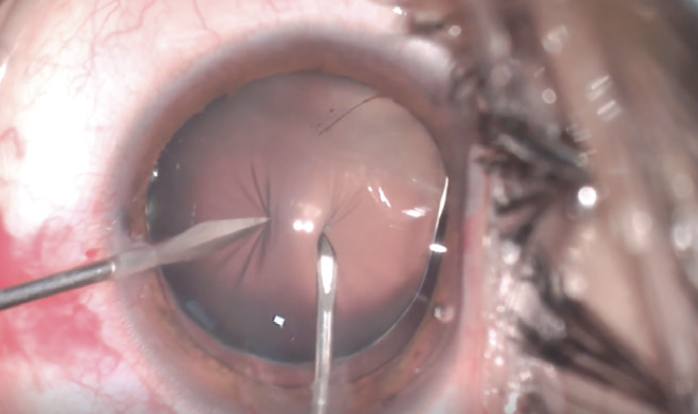
Figure 1. A microvitreoretinal blade and a cystotome facilitate capsular access.
Step No. 2. A dispersive OVD is injected into the anterior chamber. The tunnel is enlarged to 5.2 mm with a blunt keratome.
Step No. 3. Two apertures are made in the anterior capsule with a microvitreoretinal blade through the sideport and a cystotome through the main incision. These two simultaneous but opposite centripetal forces balance each other and avoid traction on weak zonules and further subluxation of the lens. The two apertures in the capsule are held by a 27-gauge cannula to support the lens, much like a straight handle on an old-fashioned bag.
Step No. 4. The capsulorhexis is completed. A 27-gauge cannula is used to hold the bag steady, hence the name bag handle technique (Figure 2). Next, 0.1 mL of 1% lignocaine is injected in the anterior chamber, on the surface, and behind the iris. Excess infusion behind the iris is avoided to prevent misdirection syndrome.
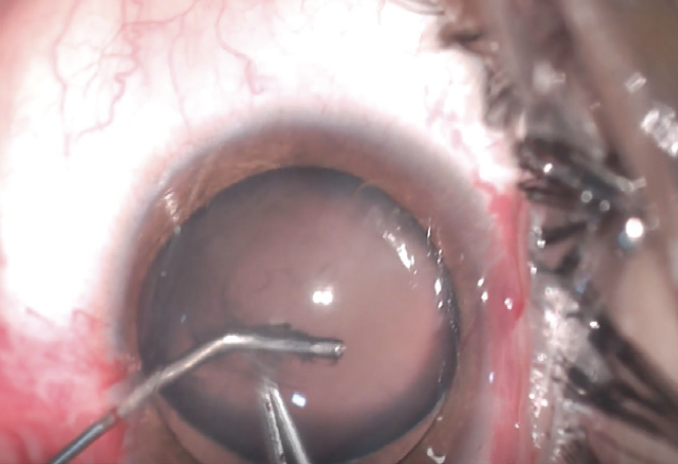
Figure 2. The handle of a cystotome is used to steady the bag.
Phacoemulsification was not necessary in the case presented in the video. Irrigation and aspiration were controlled manually with a Simcoe cannula mounted on a Simcoe bulb and a 5-mL syringe and independently with visual guidance. Surge and overdeepening of the anterior chamber must be avoided. The IOP remains in a normal range throughout the procedure. In the case presented in the video, 0.2 mL of pilocarpine 0.5% was infused into the anterior chamber to achieve a 4-mm pupil. An iris-claw lens was implanted in the anterior chamber (Figure 3), rotated 90º, and held at the haptic-optic junction before it was enclavated to the back of the iris (Figure 4). The maneuver was repeated on the other side. It should be mentioned that the posterior capsule is not removed, and the hyaloid face is not disturbed.
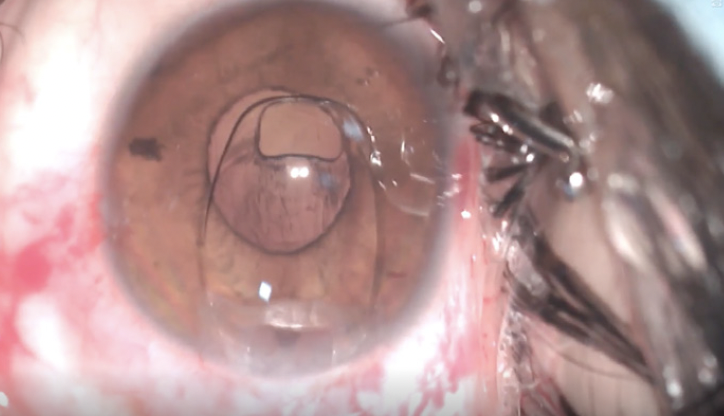
Figure 3. An iris-claw lens is implanted.

Figure 4. The IOL is enclavated in the iris.
I have been performing the bag handle technique for many years. The posterior chamber has remained clear even though the IOL is not placed inside the bag, perhaps because the large size of the capsulotomy encourages the edge of the rhexis to fibrose and seal with the opposing posterior capsule in the early postoperative period and prevent the migration of lens epithelial cells to the central posterior capsule.
POINTERS
The bag handle capsulorhexis is a low-pressure and low-fluidics manual technique. At no point will the IOP rise above the physiologic range. If the capsulorhexis tears toward the periphery, it can be easily retrieved and completed. In an eye with a soft lens, hydrodissection and hydrodelineation can be performed segmentally, and the entire lens can be aspirated with a Simcoe I/A cannula. The irrigation and infusion are controlled independently with visual feedback from the microscope to avoid surge and high pressure.
An IOL can be placed in the capsular bag with scleral fixation and capsular tension rings or, after a vitrectomy, in the anterior chamber, with scleral fixation, or, as in this case, an iris-claw lens fixated to the back of the iris.
The advantages of the safe and quick bag handle technique are topical anesthesia, capsular bag retention, an intact hyaloid face, and a zone of pars plana. Immediate rehabilitation without a patch is important for good long-term results.
1. Steinert RF, Fine IH. Cataract Surgery: Technique, Complications & Management. 1st ed. Saunders; 1995.
2. Kwitko ML, Kelman CD. The History of Modern Cataract Surgery. Kugler Publications; 1998.
3. Gimbel HV. The history of the capsulorhexis technique. Cataract & Refractive Surgery Today. October 2007;7(10):39-41.

