
“Healthcare organizations need to face the reality that they’re competing for hearts, minds, and dollars the same way any other business has to. We don’t and can’t win in any market competing as we did in the past.”
— Ken Schmidt, brand visionary
“Change before you have to.”
— Jack Welch, former Chairman and CEO of General Electric
Heed the warnings of Ken Schmidt and Jack Welsh, and change now before you have to. Otherwise, by the time you realize change is inevitable, it may be too late.
In general, patients are becoming more astute, aware of their options, and judicious about who provides their care. This has never been truer for ophthalmology than now, especially considering the number of procedures that require high out-of-pocket costs such as premium lens replacement.
Prospective candidates who seek to reduce or eliminate spectacle dependence are discerning. Surgeons with a strong, well-established reputation for delivering a broader range of vision as their standard of care are poised to capture these patients’ business. Conversely, it is too costly and time-prohibitive for doctors who offer general services and only dabble in premium lens procedures to compete. Market Scope estimates that, in the few years since being introduced to the market, enhanced monofocal IOLs already represent 5.5% of manufacturer revenue in the premium IOL category (Figure 1).1 If this growth rate continues, today’s premium monofocal IOLs may easily become tomorrow’s standard monofocal IOLs, leaving surgeons who mainly provide general services in an undifferentiated and messy middle. Facing a proverbial crossroads, they will be left to choose between adopting a refractive mindset or risking losing their premium lens business to a competitor. For surgeons daring to differentiate themselves from other practices, now is the time to make the necessary changes.
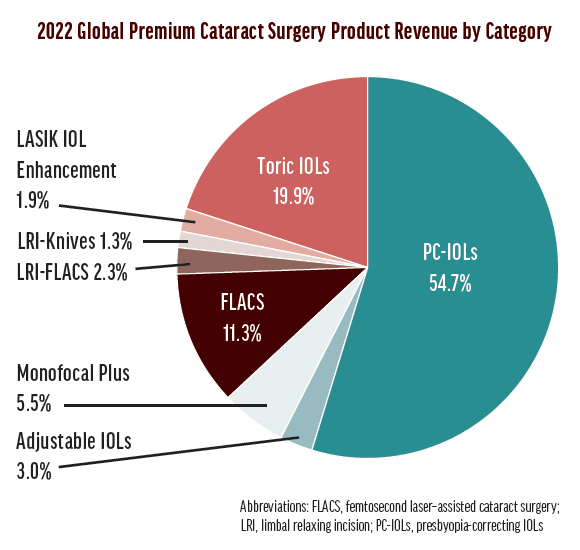
Figure 1. Product revenue by category in the global premium cataract surgery sector. Source: Market Scope
TRUST AND REPUTATION
As my friend and the principal and managing director of the health care marketing firm Feed. The Agency, Matthew Ray Scott, says, “Trust is your currency, and reputation is your bank account.” Most patients can’t critically evaluate your surgical skills and knowledge or the technologies you use, so they judge the quality of care you deliver based on things they have a frame of reference for, such as the environment and the experiences they have engaging with you and your team. Every interaction either deposits or withdraws trust.
When it comes to lens replacement procedures, there are three things you can do to grow your reputational wealth.
No. 1: Change your practice mindset. A surgeon-centric practice is outdated. Modern patients expect a hero’s journey on their quest for better vision. Like Luke Skywalker’s path in Star Wars, the frustrated presbyopic patient (with or without cataract) is also searching for knowledge, dreaming of a life without glasses. These patients set out to find a surgeon-guide, rely on the staff to perform diagnostics, and learn about their options before they undergo the procedure that will result in newfound visual freedom.
In his book Building a Storybrand,2 Donald Miller outlined seven key concepts to define the patient journey:
✓ Position the patient as the hero. (You are not the hero.)
✓ Define the patient’s problem and their specific needs.
✓ Be the patient’s guide to understand their personal best solution.
✓ Create a clear plan for delivering their vision.
✓ Make a specific treatment recommendation.
✓ Discuss the potential for failure and/or drawbacks.
✓ End the patient’s journey to vision freedom with success.
No. 2: Prioritize performance, not pathology. I am the strategic advisor at ADVALIA Vision. Our surgeons and staff don’t ask patients, “What’s the matter with you?” Instead, they ask, “What matters to you?” The small difference in wording separates a refractive-minded surgeon from their competitors. The first question prioritizes the problem whereas the second prioritizes performance and helps convey to patients that the treatment plan is customized based on their personal, unique vision preferences and lifestyle needs.
Prioritizing performance also avoids the feeling of selling something to your patients. You put the patient first—their medical candidacy and preferences—and simply try to match their performance expectations to the procedure or product that is most likely to deliver the desired outcome.
If no compromise was associated with IOL cost and performance, all patients undergoing lens replacement would choose a lens that provides the broadest range of vision. Our decision tree therefore starts with the IOL that delivers the greatest range of vision and downgrades in a stepwise fashion based on candidacy and suitability until we find the best solution for each patient (Figure 2). Adopting the mindset of downgrading versus upgrading IOLs has been the single most important factor driving the volume of presbyopia-mitigating procedures in our practice.
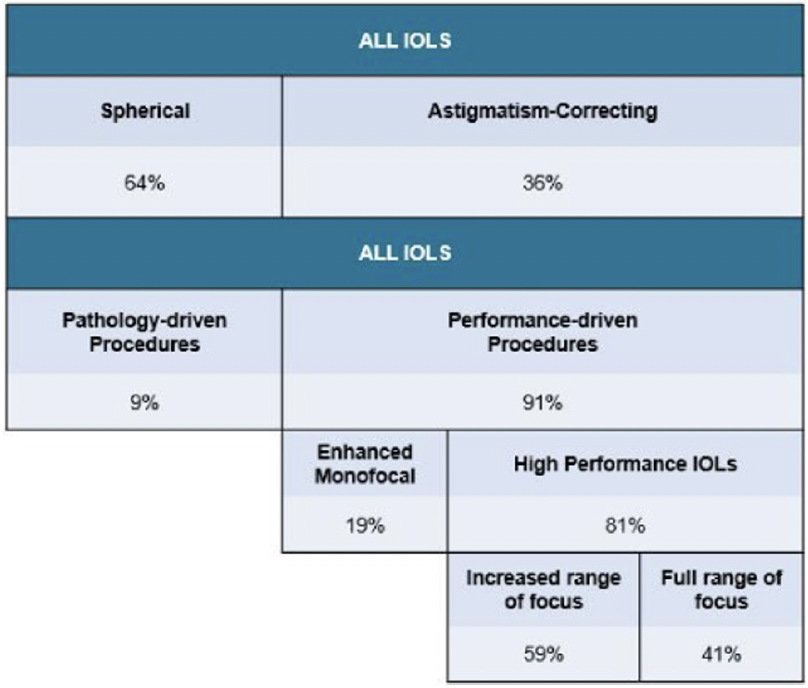
Figure 2. ADVALIA Vision’s IOL decision tree.
No. 3: Optimize your patient flow. Patient flow is key to providing an exceptional patient experience. The following strategies can be effective.
- Complete all diagnostics before you see the patient. Many surgeons are hesitant to perform advanced diagnostics before knowing if patients are interested in a presbyopia-correcting IOL. A surgeon’s time is the most expensive resource in the clinic, however, and it’s faster, easier, and more cost-effective to complete all diagnostic exams before meeting with patients. This strategy avoids the risk of embarrassment from making a recommendation before knowing a patient is not a suitable candidate. It also allows extra time for the staff to understand a patient’s individual needs and establish the value that a presbyopia-correcting IOL can offer to them.
- Consider your staff as an extension of you. Research shows that surgeons’ communication skills decline as they progress through their education and career.3 Let your staff help you build a better and stronger rapport faster with patients. Have them open the conversation with patients about their vision preferences, lifestyle needs, and willingness to accept compromises.
- Give your technicians autonomy. If your technician observes something during a diagnostic workup that questions a patient’s candidacy for certain treatments, make sure they have the autonomy to add exams when they feel it’s necessary. The more information you have when you see the patient, the more precisely you can make a specific treatment recommendation.
- Educate, educate, educate. Every step in the patient journey must be seen as an opportunity to educate them. Providing patients with information about their options before the visit can set the stage, but don’t underestimate the importance of an in-depth, one-on-one conversation to understand their needs and expectations fully.
- Ensure a smooth handoff at each step. You treat eyes every day. To patients, however, vision correction is a once-in-a-lifetime event that can be intimidating. Remember, each patient is the hero in their vision correction journey, and you are simply their guide. Personal handoffs from one staff member to the next can help ease a patient’s fears and be another opportunity to explain each step of the process.
- Make a clear and specific recommendation. Your patients chose you for a reason, and they trust you to help them see better. Once you have evaluated their ocular health and understand what is important to them, it is your duty to recommend the treatment option that will best suit their individual needs. You are the expert, not them. Be clear and specific with your recommendation.
- Become the specialist of your specialty in the minds of your ideal patients. Think of the saying, “a jack of all trades, master of none.” You can’t be all things to all patients. Define your ideal customer—patients with cataracts, frustrated presbyopic patients (with or without cataracts), any patient seeking to reduce spectacle dependence—and build your practice around them.
In the past, patients chose care providers based largely on referrals from friends and family. Today’s patients—especially middle-aged patients—are much more sophisticated than their parents were. They turn to the internet to find out who you say you are, who your patients say you are, and who Google says you are. Critically reflect on the following:
- Am I interesting from a prospective patient’s point of view?
- How am I differentiated from my competitor?
- How can I be perceived as the specialist of my specialty?
Patients who are interested in a presbyopia-correcting IOL don’t start their search looking for a full-service ophthalmologist. They are looking for someone who specializes in providing better vision. Your practice mindset, the patient experience you deliver, and, ultimately, the outcomes your patients achieve will prove who you are. Your ideal prospective patients must perceive you as being No. 1 in your specialty. There will always be other surgeons who have more surgical experience, use newer technology, or charge less than you. The bottom line is this: Better is not better; being different is better.
CONCLUSION
In January 2020, ADVALIA Vision opened a new clinic with the space and office design that allowed the practice to grow its reputational wealth using the steps outlined in this article. During the past year, the practice’s surgical volume was 74.5% above its 2019 volume, the previous practice record. Most lens replacement patients (91%) received a presbyopia-mitigating IOL, and a laser-assisted cataract surgery technique was used in 99% of those cases.
1. 2022 Premium Cataract Surgery Market Report: Analysis of the Top 13 Countries for 2021 to 2027. Market Scope. November 2022. Accessed February 10, 2023. https://www.market-scope.com/pages/reports/346/2022-premium-cataract-surgery-market-report-analysis-of-the-top-13-countries-for-2021-to-2027-november-2022
2. Miller D. Building a StoryBrand: Clarify Your Message So Customers Will Listen. HarperCollins Leadership an imprint of HarperCollins; 2017.
3. Ha JF, Anat DS, Longnecker N. Doctor-patient communication: a review. Ochsner J. 2010;10(1):38-43.

