


Keratoconus is particularly aggressive in individuals who are in their teens and 20s. If the disorder remains untreated, patients may sustain vision loss and require a corneal transplant. Before CXL was developed, corneal transplantation was ultimately required by 11% to 27% of individuals with keratoconus.1 Early diagnosis and treatment are crucial to preserving the vision of people who have the disease. A compassionate act by Glaukos helped to save the vision of one of my young patients with keratoconus.
CASE PRESENTATION
A 27-year-old woman experienced rapid refractive changes and was diagnosed with keratoconus. At the initial evaluation, topography showed an obvious cone. The maximum keratometry (Kmax) value was 52.10 D (Figure 1). The patient’s BCVA was 20/20, but I considered her to be at risk of disease progression and vision loss. Six months later, topography documented significant progression, and the Kmax value was 54.30 D (Figure 2). The patient’s BCVA remained 20/20.
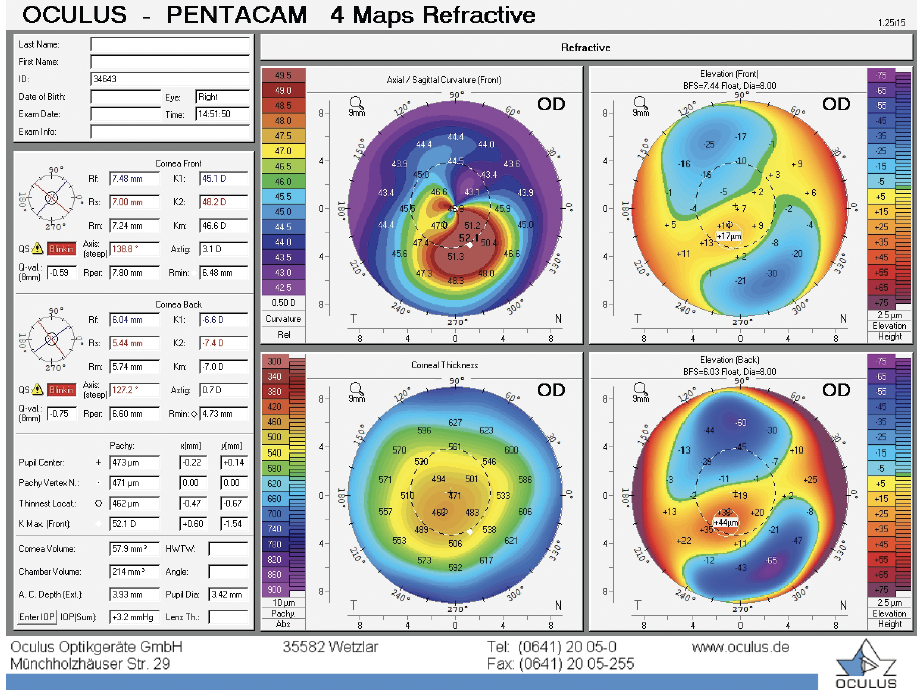
Figure 1. Images obtained at the initial presentation.
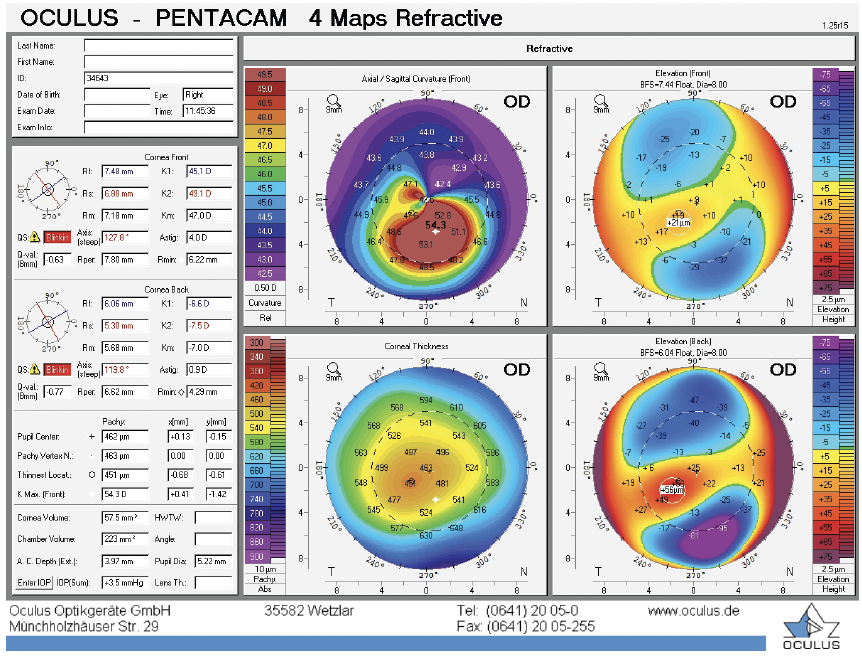
Figure 2. Images obtained 6 months after the initial presentation shows disease progression and an increase in the Kmax value.
I recommended CXL to prevent vision loss and further disease progression. Unfortunately, the patient lacked insurance coverage to pay for treatment and could not afford to pay for the procedure herself. CXL is expensive; the cost of riboflavin alone is more than $3,000.
I contacted Glaukos, and the company agreed to provide riboflavin at no charge to the patient. She underwent CXL. Nine months after treatment, the Kmax reading was 53.80 D (Figure 3), and her BCVA was 20/20.
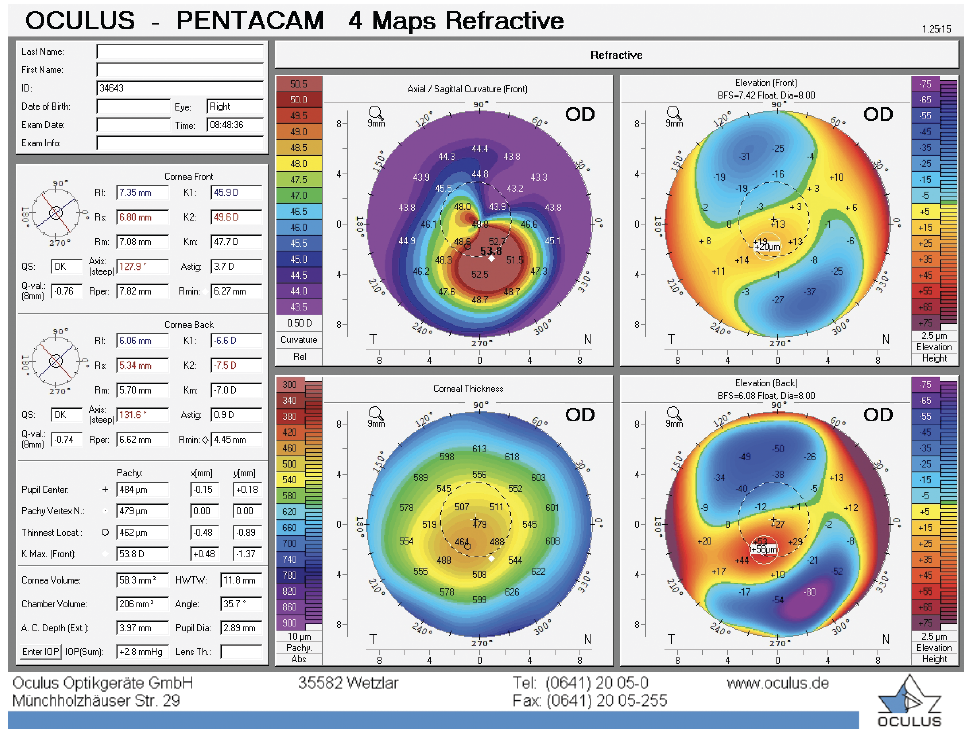
Figure 3. Images obtained 9 months after CXL shows a decrease in the Kmax value.
CONCLUSION
As this case demonstrates, compassionate acts by industry can benefit patients with ophthalmic diseases. Flattening the patient’s cornea and stabilizing her refraction improved her chances of retaining vision and avoiding a corneal transplant in the future.
1. Beckman KA, Gupta PK, Farid M, et al; ASCRS Cornea Clinical Committee. Corneal crosslinking: current protocols and clinical approach. J Cataract Refract Surg. 2019;45(11):1670-1679.

