


Greater Patient Satisfaction Requires Proper Diagnostic Testing and Setting Reasonable Expectations
Natalie Afshari, MD, FACS

Thorough preoperative planning is essential to achieve excellent outcomes in refractive cataract surgery. Proper diagnostic testing and counseling to help set reasonable expectations ultimately lead to greater patient satisfaction. In my practice, the preoperative evaluation begins with a thorough history, a complete ocular examination with an emphasis on the ocular surface, a manifest refraction, and a determination of ocular dominance.
Planning for astigmatism management is a key component of a complete preoperative evaluation. My staff and I routinely measure astigmatism using multiple modalities, including the manifest refraction, the Pentacam (Oculus Optikgeräte), and the IOLMaster (Carl Zeiss Meditec). It is important to look for concordance between the power and axis of astigmatism with these modalities. If a discrepancy is found, we look for pathology that can affect astigmatism such as dry eye disease. Patients who have irregular astigmatism generally are not good candidates for a toric IOL, and we tend to recommend a rigid gas-permeable contact lens trial (over-refraction to determine BCVA).
TARGET REFRACTION
A thorough discussion of the target refraction with patients is a key part of surgical planning. The target refraction should take each patient’s lifestyle and hobbies into account. Patients oftentimes are not familiar with the limitations of current lens technology and expect to achieve the vision they had in their youth. For example, patients with -2.00 D myopia may be unaware that, after cataract surgery with a distance target, they may no longer be able to read at near without spectacles. Many of these patients prefer to retain their near vision postoperatively. When patients prioritize distance vision, we generally have them perform a trial of their postoperative vision using trial lenses. Most patients choose distance correction and understand that they will need reading glasses after surgery.
Monovision is a great option for patients who desire a degree of spectacle independence, but caution should be exercised when they have no prior experience with this corrective strategy. We frequently have patients perform a monovision trial in the clinic or for a short time at home to see how well they tolerate it. Occasionally, dense cataracts will prevent a full demonstration of monovision.
There are different degrees of monovision, but a target refraction of -1.50 D in the nondominant eye is often well tolerated and efficacious for computer use and some reading vision. Regardless of the degree of monovision, we inform patients that they may need to wear glasses for some tasks even after perfect surgery.
OCULAR DOMINANCE and PRIOR REFRACTIVE SURGERY
We routinely check ocular dominance and operate on the nondominant eye first if the cataracts are symmetric. Preoperatively, we also hold a 0.50 D lens in front of the nondominant eye to simulate the effect it would have at near; this strategy works best in patients who do not have a dense cataract.
A history of refractive surgery makes accurately calculating IOL power more challenging. Many of these patients expect the precision of laser corneal ablation, so setting realistic expectations is particularly important. We stress that they may have a residual refractive error after cataract surgery that may require correction with spectacles, contact lenses, or additional surgery.
I routinely perform intraoperative aberrometry in these cases, and I use advanced IOL formulas such as the Barrett True K to optimize outcomes. In patients who previously underwent hyperopic LASIK, I recommend an IOL with neutral spherical aberration and target slight myopia.
The irregular corneal astigmatism of patients with a history of radial keratotomy poses a unique challenge when premium lenses are requested. In some cases, scleral lenses may be the best option for optimizing vision.
PREMIUM LENSES
We always counsel patients who elect a premium IOL on the risk of postoperative glare and halos, and we screen them preoperatively for macular pathology with macular OCT. The higher cost of these lenses raises patients’ expectations. We emphasize that they will not be free of spectacles 100% of the time after surgery. We also thoroughly discuss the risks and benefits of surgery, including the possible need for an enhancement.
The 90-Minute Cataract Evaluation
Dain Brooks, MD

Looking toward the future of cataract surgery, many ophthalmology clinics are shifting to a more efficient, premium patient experience. In a nutshell, we need to see more patients in less time and help them understand the benefits of advanced technology IOLs.
Our practice has one surgeon and two optometrists. We conduct an average of 20 cataract evaluations daily and perform approximately 70 surgeries a week; the majority of our patients choose an advanced technology lens. We’ve streamlined several processes to achieve these levels, and we are always pressing forward to improve the patient experience and our outcomes.
The biggest shift in our patient experience has been what we call the 90-minute cataract evaluation. This concept grew out of necessity; our clinic has grown rapidly and required structure. We came up with a system that allows us to work efficiently, maximize the quality of time we have with our patients, and decrease patients’ fatigue at the end of the evaluation. The 90-minute cataract evaluation has also helped us to increase patients’ interest in advanced technology IOLs.
THE PLAN
Once we knew approximately how long an evaluation should take, we then determined how many patients we could reasonably see in a clinic block and how we needed to staff the clinic.
We divide our technician staff into two teams, which we call the diagnostic department and workup department. The diagnostic technicians are responsible for testing and calculations. Having the same staff members perform the same tests improves the accuracy and precision of our measurements because they know how to get the best scans quickly.
We also limit the number of tests performed during the evaluation. We now perform only topography (OPD-3, Nidek) and OCT of the macula and retinal nerve fiber layer. These measurements help me determine how much astigmatism needs to be corrected, the size of the pupils as it relates to a pinhole effect or halo concerns, the health of the macula, and signs of underlying glaucoma. If glaucoma is a concern, I often plan a combined cataract/MIGS procedure. These tests also help me quickly and accurately determine the patient’s candidacy for advanced technology IOLs.
COMMUNICATING WITH PATIENTS
The other part of successfully implementing the 90-minute cataract evaluation is the discussion with patients. The more involved patients are in customizing the treatment plan, the more interested they become in advanced technology IOLs. Listening to their vision goals and making a strong lens recommendation based on their ocular health and lifestyle is crucial. We have found that we don’t need to spend more than 5 to 10 minutes with patients to understand how best to fix their problems.
Timing is everything in the 90-minute cataract evaluation. As I wrap up the discussion with patients, our scribe messages a counselor to join us in the examination room. The counselor listens to the last part of the conversation and moves the discussion in a natural way to their office for scheduling. This segue keeps me from running behind and allows patients to move along in the process. We have three counselors to ensure patients don’t have to wait to schedule surgery or discuss insurance questions.
CONCLUSION
Your patients value their time as much as they value yours. If patients spend 3 to 4 hours in your office for an evaluation, by the end, they are likely tired, hungry, and ready to leave. By taking steps to decrease the time it takes to complete the initial cataract surgery evaluations, patients will leave your office feeling energetic and excited about gaining the vision they have always wanted.
Three Key Considerations for Optimizing Patient Care
Nicole R. Fram, MD

The cataract patient journey starts with the first impression. Patients feel a tremendous amount of anxiety about their vision as well as COVID-19, so how my staff and I alleviate those issues are paramount to the visual rehabilitation process.
STREAMLINING INTAKE
The only blessing of the COVID-19 pandemic in our office has been the implementation of a prefill call for all new patients to decrease office time and the chance of exposure. A phone call is made 1 to 2 days before the scheduled visit, at which time the chief complaint, medical history, patient questionnaire responses, medications, allergies, and insurance information are all entered into the patient's chart. Additionally, patients receive an email with information and links to educational videos explaining cataract surgery (Figure 1), if applicable. Lastly, patients are prepared in advance that the preoperative visit with biometry can take up to 2 hours, which facilitates realistic expectations and preparation. With this prefill, patients’ overall time in the office is reduced, preoperative testing is expedited, flow is efficient, and patients feel cared for and safe.
Figure 1. Information and educational videos can be sent to patients before and after their appointments to assist with cataract surgery counseling.
TESTING
The following are performed before patients enter the exam room: refraction, glasses prescription check, autorefraction, biometry, iTrace (Tracey Technologies), corneal topography, macular OCT, Retinal Acuity Meter (AMA Optics), and glare tests. If corneal topography reveals an irregular Placido disc image, the technician alerts the doctor, pupillary dilation is deferred, and the ocular surface is carefully evaluated and managed.
During the examination, critical findings such as dry eye disease, epithelial basement membrane disease, corneal guttae, degree of pupillary dilation, anterior chamber depth, quality and density of the cataract, and the presence of pseudoexfoliation are noted. These pertinent findings help to determine the order of cases on the day of surgery and signal whether extra time and/or counseling is required (Figures 2 and 3).
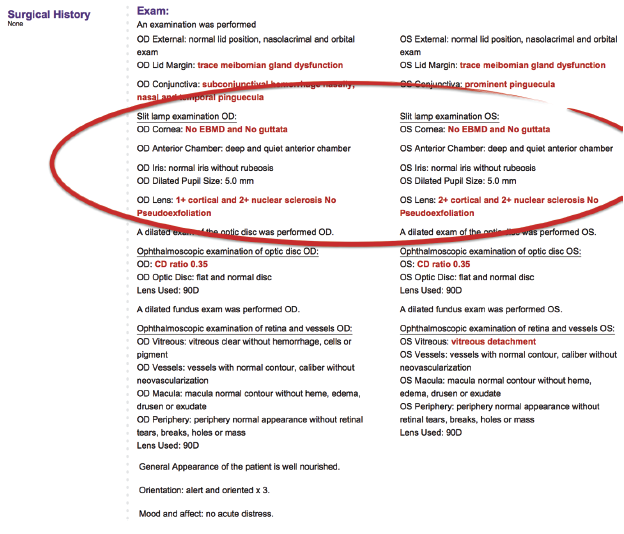
Figure 2. The documentation of pertinent positives and negatives assists with cataract surgery planning, such as the order of cases and time blocking.
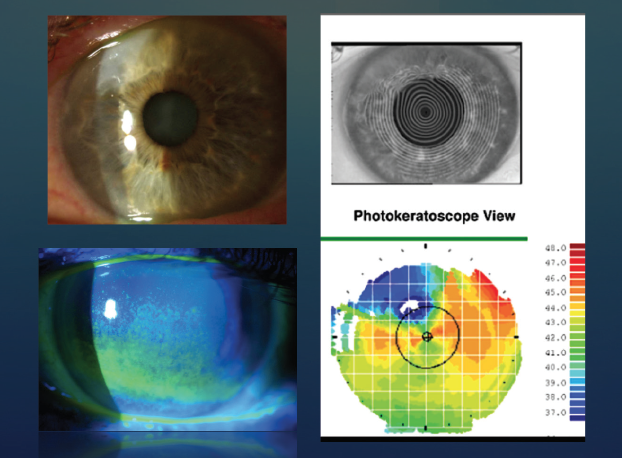
Figure 3. Slit-lamp photographs of a Salzmann nodule (top left) and punctate epithelial staining from dry eye disease (bottom left). Corneal topography shows irregular astigmatism and superior flattening from a Salzmann nodule (bottom right). A thorough examination of the ocular surface and corneal topography with Placido imaging helps to determine if a patient is ready for cataract surgery or if additional treatment to optimize the ocular surface is required.
IOL SELECTION
During the examination. I use a separate screen to display test results and educate patients in real time about their ocular anatomy. It is at this point in the examination that I ask patients about their lives, occupations, work, hobbies, and goals. I take this information into account when recommending the best technology to meet their needs safely. I explain that all IOL technologies have drawbacks and that their anatomy and preexisting conditions may dictate the best choice. For example, a patient with an epiretinal membrane or age-related macular degeneration is generally not a candidate for a diffractive technology in our practicep>
Surgical planning begins in the room. I review the corneal topography and biometry before I begin a discussion of astigmatism correction with patients, during which I also assess their willingness to wear spectacles. If they have more than 0.75 D against-the-rule astigmatism or more than 1.25 D with-the-rule astigmatism, I often recommend a toric IOL to achieve the best quality of uncorrected vision.
The availability of trifocal and extended depth of focus IOLs has caused a major shift in how we recommend lenses to patients in our practice. We find that these lenses are performing well compared to previous generations of presbyopia-correcting IOLs. These current IOLs are finally meeting patient expectations and are associated with fewer nighttime diffractive dysphotopsias. We refer to these IOLs as lifestyle lenses. However, we emphasize that these IOLs are not perfect but generally give patients a great degree of spectacle independence. We perform an evaluation of higher-order aberrations such as coma and angle kappa to identify patients who may have trouble with diffractive IOL technology. Throughout the IOL selection process, I reassure patients that an IOL exchange will be performed if they cannot tolerate a given technology.
The Light Adjustable Lens (RxSight) has also increased our success in achieving on-target, customized, and quality vision in patients with a history of successful monovision and those with a history of LASIK or radial keratotomy. In the past, IOL calculations after LASIK and radial keratotomy were daunting and required a tremendous amount of patient counseling regarding outcomes. After implementing the Light Adjustable Lens, the targeting is rarely an issue and quality of vision is significantly improved.
After the examination. My first assessment of the test results is quality control. When evaluating corneal topography, I look at the quality of the Placido image and the regularity of the astigmatism. Next, I evaluate the amount of astigmatism while focusing on the reproducibility of both power and axis with at least two technologies. Biometry also has quality control measures with regard to the signal ratio, keratometry (K) readings, and a posterior segment OCT scan (IOLMaster 700; Figure 4). When a toric IOL will be implanted, I use the Barrett integrated K readings, Barrett Toric Calculator (Figure 5), and the biometry-suggested K readings (Figure 4, top right).
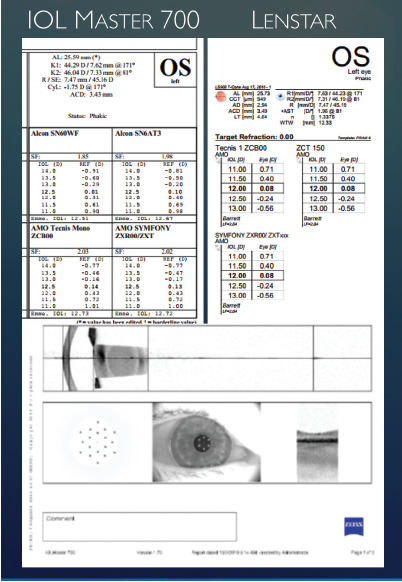
Figure 4. Preoperative biometry using the IOLMaster 700 with swept-source OCT, keratometry quality, and macular OCT (top left and bottom). Recommended K readings and integrated toric IOL recommendation on the Lenstar (Haag-Streit, top right).
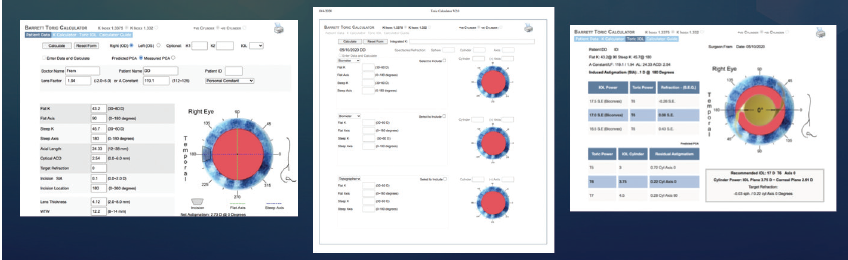
Figure 5. The Barrett Integrated Keratometry screen allows the integration of multiple K readings, which can improve the accuracy of toric IOL selection.
We recently began using Veracity Surgical (Carl Zeiss Meditec) in our practice to help streamline surgical planning. This software displays innovative methods of IOL calculation such as the Barrett True-K and Hill-RBF formulas and integrated K readings (Figure 6). The software also allows me to change the target without going back to the biometer and printing out new calculations. The staff and patients appreciate this prepared approach.
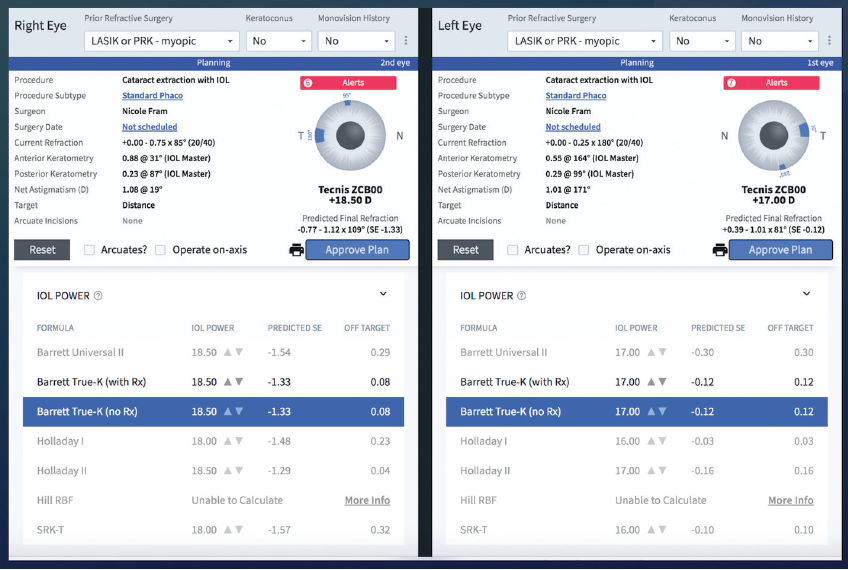
Figure 6. Veracity Surgical can help to streamline IOL calculation and selection.
Figures 1–6 courtesy of Nicole R. Fram, MD
CONCLUSION
A thorough evaluation, compulsive testing, and a streamlined process allow us to optimize patient care. We are reminded every day that it is a privilege to care for our patients. The more thorough and efficient we make the process, the better our outcomes.
Surgical Planning in 10 Steps
Ivan Gabrić, MD

Svjetlost is an ophthalmology chain of six centers in Southeastern Europe with more than 200 employees and 70 ophthalmologists. It is a challenge to ensure that the quality of care and patient experience are optimal across the board. On average, more than 10,000 eye surgeries are performed at our centers per year; of these, approximately 4,000 are laser vision correction procedures, and approximately 3,000 are refractive lens surgeries. Maintaining an excellent standard of care requires executing many carefully planned steps.
MARKETING
Surgical planning starts before patients arrive for their first appointment. The trick is in the marketing. I have heard many doctors complain that it’s hard to recruit patients from their general practice to undergo refractive procedures. Almost 100% of our refractive surgery patients arrive wanting refractive surgery because they have seen our marketing materials.
Through those efforts, patients come to our offices already knowing which procedure they want and the expected end result. We don’t have to convince them of the merits of the refractive surgical procedures we offer.
This approach is preferable to the following scenario. A 60-year-old patient wearing presbyopia-correcting glasses presents for a routine eye examination. The doctor and staff attempt to convince the patient to undergo refractive lens exchange. They spend an enormous amount of energy on the effort. The patient undergoes the procedure. A problem is encountered later, and the doctor and staff are blamed for corralling the patient into surgery.
10 STEPS
A compelling marketing campaign promotes the benefits for patients. We don’t sell excimer laser surgery or multifocal IOLs. Instead, we promote the improvement in quality of life that patients can expect after surgery, and we do it in 10 steps.
Step No. 1: Contact. Once patients decide a procedure or technology is something they want, they contact the office. Our staff is familiar with the basics of patient selection for each offering, so they can make a preliminary determination of candidacy and respond appropriately to patients. Pricing is also made clear from the outset so that patients will not waste their (and our) time if they can’t afford the desired procedure.
Step No. 2: Timeliness. As a rule, all examinations are performed within 7 days of patients’ first calls for an appointment. Longer waits can decrease their level of motivation.
Step No. 3: Testing. Patients have a brief conversation with a doctor, who assesses their needs and wishes and orders the examinations that should be performed. Generally, patients receive multiple objective examinations. For example, if they are interested in and are candidates for laser vision correction, they undergo corneal analysis with the Pentacam, aberrometry, topography, axial length measurement, OCT, and a full ophthalmologic examination. Patients who are interested in and candidates for IOL surgery receive this same battery of tests in addition to ultrasound, specular microscopy, and IOL calculation.
Step No. 4: Review of results. The doctor reviews the results of all the objective tests before patients return. As a result, the doctor is aware of which options are most suitable and can better guide the consultation.
Step No. 5: Consultation. The benefits and compromises of each option are explained to patients. We never promise what we will not be able to deliver. We follow the common credo: Underpromise and overdeliver.
Step No. 6: Scheduling. Surgery is scheduled as soon as possible, again to keep patients’ motivation high.
Step No. 7: Bilateral surgery. For lens-based surgery, we perform immediate sequential bilateral cataract surgery in 95% of cases because it is easier for patients to organize their work obligations around a single recovery period. To prevent infection, all draping, gloves, and instruments are changed between eyes.
Step No. 8: Postoperative day 1. To promote patient confidence and satisfaction, our goal is for their visual recovery to be 90% complete by their visit on postoperative day 1.
Step No. 9: Postoperative day 7. Our goal is for more than 99% of patients to return to their daily routines with minimal limitations by this visit.
Step No. 10: Enhancement. If a refractive surprise is encountered with refractive laser or lens surgery, all enhancement procedures are performed in-house at no cost to the patient.
CONCLUSION
At Svjetlost, we perform about 10,000 procedures per year. A 1% complication rate potentially would equate to 100 unhappy patients each year. We have been in business for 23 years—but we have not seen 2,300 unhappy patients. This is because we have optimized our processes so that our complication rate is below 0.1%. Even when a complication does occur, we correct it quickly and at no additional cost to the patient.
Lens Choice Is an Important Consideration
John A. Hovanesian, MD

The importance of preoperative planning in cataract surgery should not be underestimated. Innovations that help me to improve efficiency and enhance surgical planning and outcomes are welcome additions to my workflow. Most recently, I have integrated a cloud-based surgical planning app that allows me to transfer preoperative measurements and data between the clinic and the OR.
The Smart Cataract Planner app (Alcon) is used mainly to help deliver optimal postoperative outcomes with the company’s IOLs. This tool enables me to streamline the back-office work, integrate measurements from multiple diagnostic devices, incorporate patient lifestyle information, and analyze and optimize my plan for surgery (Figure 7). The app has an eleven-box grid of different lens implant options that facilitates my consideration of a variety of IOL options based on target refraction, design, and power and helps me to determine how each would affect the predicted outcome.
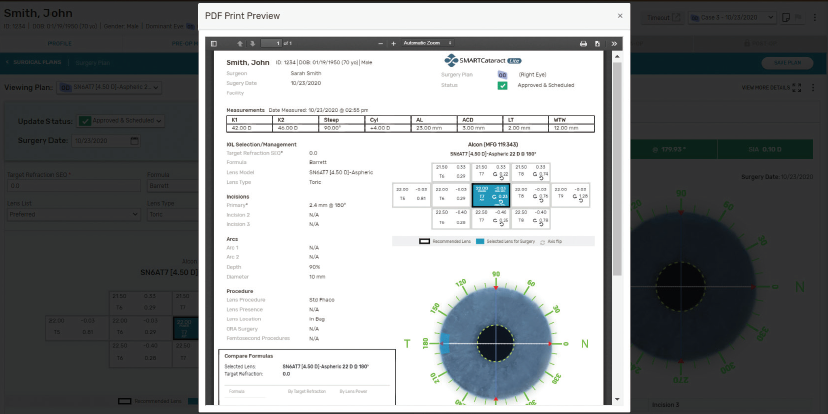
Figure 7. PDF print view of a Smart Cataract Planner surgical plan.
Courtesy of Alcon
Built-in toric calculators on the Smart Cataract Planner app also help me to optimize cylinder correction. More than 70% of my patients have 0.50 D or more of astigmatism and receive a toric IOL. Having instant access to all of the most advanced formulas streamlines IOL calculations and eliminates the need to transfer data by hand from another website or software.
I also appreciate that the app is customizable. Because I work with a group of 16 doctors, the ability to create preferences and save them in the Smart Suite is essential.
CONCLUSION
Ultimately with cataract surgery, we surgeons are not after diopters—we're after happy patients. The Smart Cataract Planner app allows me to plan surgery while keeping patients’ needs in mind. It also improves the patient experience by helping me to think ahead.
Three Keys to Practice Efficiency
Florian T.A. Kretz, MD, FEBO

Optimizing processes is the key to continuously improving outcomes. If this wasn’t clear before, it certainly has become so during the COVID-19 pandemic. I perform surgery at three different centers. Proper time management, surgical planning, and workflow optimization are essential to my ability to complete my schedule, run the businesses, conduct research, and spend time with my family.
PROPER TIME MANAGEMENT
Both my time and patients’ time must be managed. Before the current pandemic, my staff and I monitored the time required of patients for each treatment, procedure, and diagnostic test, but analysis stopped when patients finished this process rather than when they left the building. Spatial restrictions related to COVID-19 prompted us to limit how long a patient is permitted to be in each clinic area and designate a departure time. This change has dramatically increased practice efficiency.
After successful cataract or refractive surgery, patients leave the OR, receive counseling, and exit the facility with a paper bag filled with a drink (water, sparkling wine, or beer; Figure 8), a sandwich, sunglasses, and postoperative instructions. Two hours later, they receive a phone call to confirm that they understand all of the information provided, ask if they are experiencing problems, describe what to expect during the next 24 hours, and confirm their follow-up appointment for the next day.

Figure 8. Patients treated at Dr. Kretz's clinics receive a beverage of their choice with a custom label.
SURGICAL PLANNING
Surgical planning is probably the process that changes most frequently at our facilities. Incoming patients are treated by a team of technicians and counselors. The technicians make sure that the measurements are accurate. The counselors find the surgical procedure or IOL choice for each patient depending on individual needs. Afterward, technicians calculate all parameters for the surgery, such as IOL power, toricity, and ablation zone for laser vision correction procedures. The patient and data are presented to the doctor, who can change the parameters online during the examination and who confirms the decision at the end. No printouts are required because everything is online and saved in the electronic medical record (EMR) system. Next, supplies are ordered, and the data are transferred to the OR. I receive a notification, usually by telegram messenger or email, to log into a virtual private network to review and confirm the case if a second opinion is needed.
The implementation of Forum and EQ Workplace (both from Carl Zeiss Meditec) has been enormously helpful for our clinics in northwestern Germany. All of our devices manufactured by the company are connected here. IOL calculations can be performed directly in the software, and the necessary data are sent to the Callisto eye (Carl Zeiss Meditec). In southern Germany, we use custom software to import patients’ diagnostic data, calculate IOL power and astigmatic correction, and account for surgically induced astigmatism through positioning of the cataract incision. Full online integration of patient data makes changes quick and repeatable and saves time.
WORKFLOW OPTIMIZATION
Another important step is grouping different surgical procedures and patients into one surgical day. The three locations where I perform surgery have completely different setups. A femtosecond laser for cataract surgery is available at each location, but they are from different manufacturers. Each OR is equipped with a different surgical guidance system and different phaco machine. This may sound crazy, but it is intentional and works well. Equipment has been selected to meet the needs at each location.
The Erlangen facility has only one OR for refractive and intraocular surgery. The OR has the Bausch + Lomb suite consisting of a Teneo excimer laser and a Victus femtosecond laser, which I also use for laser cataract surgery. Both machines stand in the back of the room, and I operate in front of them (Figure 9).

Figure 9. Dr. Kretz’s setup in his practice’s Erlangen facility.
Another reason for this setup is that these lasers have a fixed patient bed. My routine is to perform two to three cases of standard cataract surgery followed by one laser cataract surgery procedure. Patients walk through the OR to receive laser treatment. This scheduling allows the femtosecond laser to be programmed while I perform standard surgery. Also, we have to push the microscope, my chair, and the footpedals away for patients to walk through comfortably. If laser cataract procedures were performed back-to-back, we would lose a lot of time just moving the microscope, my chair, and the footpedals back into place.
The Rheine facility is different. It has four ORs, one of which is dedicated to procedures using the Lensar Laser System (Lensar; Figure 10). I switch among the other three ORs for surgery. This setup allows me to perform laser treatments in between my other surgeries. After laser treatment is complete, the staff brings the patient to one of the free ORs. Another benefit of three ORs is greater surgical efficiency because minimal changing time is required.

Figure 10. Dr. Kretz’s setup in his practice’s Rheine facility.
Figures 8-10 courtesy of Florian T.A. Kretz, MD, FEBO
CONCLUSION
In my experience, most major manufacturers offer products of similar quality. The key is to analyze the practice’s current setup and workflow and to optimize what is easy to change and adapt to.
Improvements to Our Process and Outcomes Come With Greater Efficiency
Joseph L. Parisi, MD, FRCSC, FACS

Preoperative planning is a crucial part of any surgical practice. Modern cataract surgery patients expect excellent visual outcomes, and many of them seek spectacle independence. My colleagues and I have been strong advocates of astigmatism- and presbyopia-correcting IOLs since they became available. In order to achieve excellent postoperative UCVA in our patients and to maximize spectacle independence in those who choose premium IOLs, we pay close attention to the quality of preoperative tests and measurements. We have found it is important for the surgeon not to simply delegate these tasks to a staff member, and we have found that improving our practice’s efficiency has enhanced surgical planning and outcomes.
SCHEDULING
Owing to their increasing complexity, creating surgical plans involving astigmatism and presbyopia correction can be time-consuming, especially in a high-volume practice like ours that has a goal of growing the conversion rate to premium procedures (see Increasing Premium Lens Conversions). In order to increase the efficiency of our preoperative planning process, our first step was to designate blocks of time in our schedule for preoperative cataract evaluations. Block scheduling allows our staff to focus on the tasks required for cataract patient workups without being distracted by other appointment types.
Patients are informed ahead of time of the extended length of this visit. To enable our physicians to focus on the examination and surgical recommendations, we hired and trained additional counselors to introduce patients to the available options and assess their desires, expectations, and amenability to out-of-pocket costs before their examinations. These counselors see patients again after the examination in order to finalize the physician’s recommendation, provide details such as available financing, and schedule the procedure.
During pupillary dilation, patients watch a short, customized video in which the surgeon discusses astigmatism correction, presbyopia-correcting IOLs, and laser cataract surgery. All preoperative analysis, including biometry, topography, OCT, glare testing, and a dry eye evaluation, is completed before physician engagement so that a complete review is possible. To achieve highly predictable outcomes consistently, it is necessary to invest in diagnostic technologies that provide accurate and reliable data. It is also necessary to manage dry eye disease preoperatively and to recognize the contribution of posterior corneal astigmatism.
TECHNOLOGY
Consolidating test results and clinical data in a single location for easy access and simplifying the IOL calculation process further increase efficiency. The coordination of all this information and accurate data entry are imperative.
For the past 2 years, we have been using Veracity Surgical. This software package integrates with most EMR systems (we use NextGen EMR [NextGen Healthcare Information]) and a multitude of diagnostic devices and facilitates the direct, error-free uploading of data and images for use in IOL power calculations and astigmatism planning (Figure 11). Veracity Surgical can be customized to the surgeon’s preferences. All of the required information is available in one location, and it is portable because the software is cloud-based. There is no need for a paper chart or printouts.
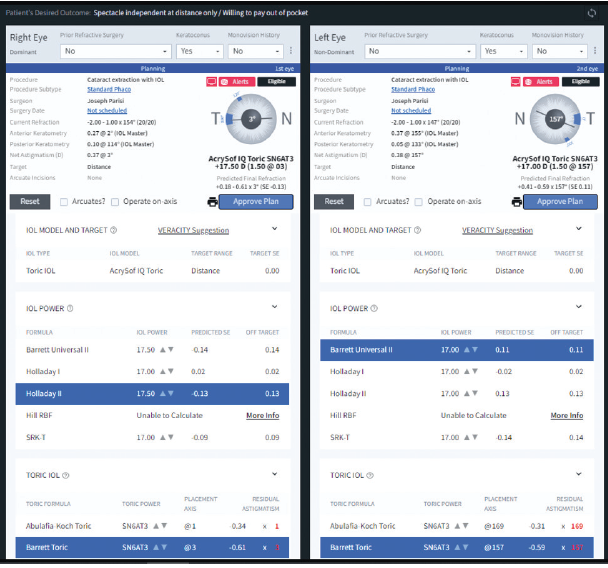
Figure 11. A screenshot of a typical Veracity planning page.
Courtesy of Joseph L. Parisi, MD, FRCSC, FACS
The software incorporates all major third- and fourth-generation IOL formulas, including the Barrett True K formula for planning cataract surgery in eyes with a history of refractive surgery. I therefore do not need to visit multiple websites to perform these calculations.
Because the software integrates with our EMR system, it alerts us to important comorbid medical and ocular conditions and tracks refractive data. The entire planning process can be performed with Veracity from any location with internet access. (Editor's note: For more on EMRs, see the article on pg 74.)
We have found the software useful during clinic flow because counselors can use the patient questionnaire to flag prior monovision experience and refractive surgery and to determine the patient’s desire for spectacle freedom and level of acceptance of out-of-pocket expenses. This information helps to streamline the doctor’s discussion with the patient during the examination. On occasion, the entire surgical plan can be finished in the lane before the patient leaves.
CONCLUSION
We have found Veracity Surgical to be especially valuable with patients coming from different clinic locations. All of the data are uploaded from each clinic and become centralized in the cloud.
My planning time is a fraction of what it used to be, and I can feel confident that the data are free of transcription errors.
Increasing Premium Lens Conversions
By Misty Brock

As a surgical counselor, I used to feel concerned about how few patients in our practice chose multifocal and toric IOLs. National market research data from Market Scope have shown that 80% of patients in the United States are interested in spectacle independence after cataract surgery and are willing to pay out of pocket for it, but adoption of this technology in our practice hovered around 10%, which is close to the national average. A change in our approach has made a positive difference for us.
EDUCATING PATIENTS
Our administrative team decided to implement new tools for educating patients, including an automated system that offers two-way communication but isn’t solely about sales. Our goal was to make our cataract surgery patients’ journeys easier by keeping them and ourselves better informed. Eventually, we chose MDbackline (MDbackline).
One of our surgeons, Clayton G. Blehm, MD, agreed to implement the software first. After a brief setup linking the software to our practice management system, MDbackline began automatically contacting patients scheduled for cataract consultations. Incoming patients received text messages and/or emails with Dr. Blehm’s name and picture in them. Upon clicking a link in these messages, patients were taken to a web service and prompted to answer simple questions about their visual complaints and desires (Figure 1). Nonbranded video- and text-based educational material customized to their responses then explained the process of cataract surgery in general, noncommercial terms.
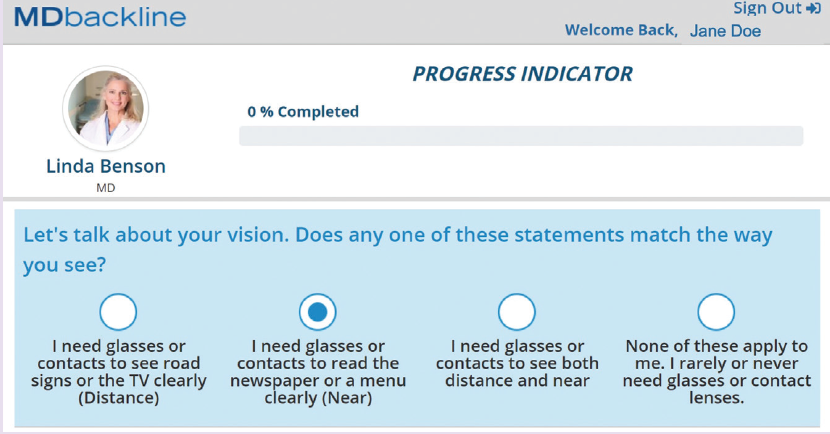
Figure 1. Questions on MDbackline are written in language at a fifth grade level. About 80% of Gainesville Eye Associates' patients respond.
CANDIDATE SELECTION
The Visual Profile Report summarizes patients’ responses and desires, identifies which of them want to upgrade to a premium product (Figure 2), and rates the likelihood that they will upgrade to premium surgery. The report also suggests which solutions may be best suited to patients and flags potential areas of concern in their responses.
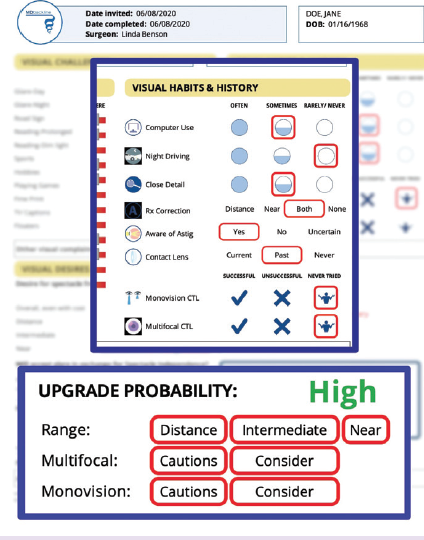
Figure 2. The Visual Profile Report guides providers and staff to IOL recommendations by providing information such as how likely a patient is to choose a premium IOL.
I use these reports when I meet with patients to guide our conversation about premium IOL options. One of my favorite features is a list of the educational material that each patient viewed, which gives me an idea of their interests and shapes our discussion. Dr. Blehm finds the personality assessment useful. The reports are included in patients’ surgical charts.
RESULTS AND FUTURE DIRECTIONS
Our practice saw an immediate bump in premium IOL adoption after implementing MDbackline. Compared to the same quarter of the previous year, premium IOL adoption jumped from 7% to more than 23%. For Dr. Blehm alone, this represented a nearly $400,000 increase in revenue after paying for the cost of the implants.
Our team is expanding our use of MDbackline to more surgeons and more functions. In addition to the aforementioned features, shortly before their cataract procedure, patients automatically receive a video in which their surgeon explains what to expect on the day of surgery. The postoperative module follows up to determine how patients are doing and invite them to give their doctor a positive review on Yelp or Google. At the end of their cataract journey, patients receive a video from our doctors thanking them for entrusting our practice with their care.
Now we are implementing the software to provide automated communication with patients who have dry eye disease and glaucoma. The Dry Eye Visual Profile Report summarizes patients’ history. It also asks them a series of simple questions in order to identify which are most likely to be interested in advanced dry eye treatment. Similarly, the Glaucoma Visual Profile Report helps to identify patients who may be interested in laser and MIGS procedures.
Automated processes that connect us more closely with patients are improving our provision of care and generating excitement about our premium services.
Take Advantage of the Digitized Care Pathway
Matthew Russell, MBChB, FRANZCO

Cataract surgery requires precise planning and execution to achieve optimal refractive results. My daily surgical planning routine for cataract surgery begins with a conversation. It is important to talk with patients about their surgical options and determine whether a premium IOL or a monofocal IOL will be implanted. We then select an implant together while still in the examination room. Because my practice has completely digitized the care pathway for patients through the use of EMRs and other technologies, I can complete this process quickly and in real time. Multiple time-consuming manual processes are condensed into simple steps with the EQ Workplace, a digital surgery planning tool.
HOW IT’S USED
In the clinic. Seamless data transfer from diagnostic devices with the EQ Workplace avoids transcription errors because the data appear in the relevant fields for IOL power calculations and IOL selection (Figure 12) without requiring manual data entry. I can also produce a PDF that can be used to order an IOL from the manufacturer.
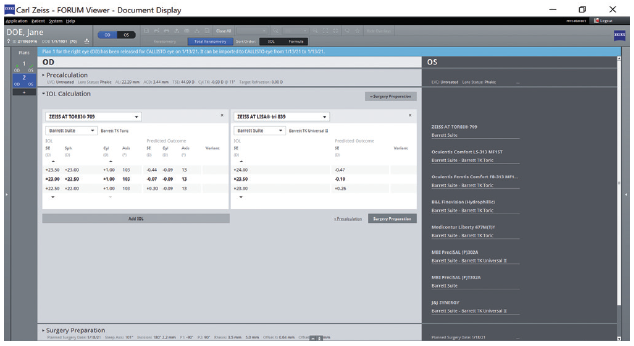
Figure 12. IOL selection with the EQ Workflow.
In the OR. EQ Workplace connects to a computer-assisted cataract surgery platform (Callisto eye) in the OR via a mobile device interface (EQ Mobile, Carl Zeiss Meditec) using a secure cloud. All relevant patient and IOL information as well as assistant functions for surgery (eg, capsulorhexis, incisions, and target axis for toric IOLs) are preset before the patient enters the OR.
I can compare the IOL in my hands with the IOL that was selected preoperatively by scanning the barcode on the IOL package. I can access all biometric and IOL data from the computer-assisted cataract surgery platform without needing to change rooms or print diagnostic readings. I use a heads-up display in the microscope to align the IOL, so I no longer need to mark the eye before surgery for toric IOL alignment.
CONCLUSION
This digitized care pathway has markedly increased practice efficiency, reduced the number of unfinished tasks that must be addressed outside of clinic time, and significantly decreased the labor costs associated with nonpatient-facing activities.
My colleagues and I are conducting a prospective study of how the use of this digital surgery planning tool (Figure 13) and computer-assisted cataract surgery platform have affected practice efficiency in the management of patients who receive toric IOLs. Our interim results show a 50% to 60% reduction in physician time and an even greater reduction in allied staff time (unpublished data, M.R.).
Figure 13. Surgery planning with the EQ Workflow.
Figures 12 and 13 courtesy of Matthew Russell, MBChB, FRANZCO
Successful Strategies for Refractive Surgery and Refractive Cataract Surgery
Karl G. Stonecipher, MD

Steve Jobs once said, “Quality is better than quantity. One home run is much better than two doubles.” Along those lines, I am a firm believer in treating every patient like a member of my family—and I have operated on my mother, mother-in-law, father, father-in-law, aunt, brother, nephews, nieces, and more. Treating patients like family steers me well, even when a complication arises. All of my patients have an opportunity to select the best I have to offer, and all of them undergo the same preoperative workup.
THE WORKUP
Every patient undergoes a 90-second workup by my staff that includes screening with the Ocular Surface Disease Index followed by fluorescein staining to evaluate tear breakup time and lissamine green staining to evaluate the conjunctiva. If the findings are positive for ocular surface disease (OSD), the consultation goes forward, but the examination is limited. Surgery is scheduled, and OSD treatment is initiated.
The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study demonstrated that many patients presenting for refractive cataract surgery have significant dry eye disease.1 The same is true of a significant number of patients presenting for refractive surgery.
REFRACTIVE SURGERY
The COVID-19 pandemic led my staff and me to change our approach to the preoperative evaluation. The wavefront and manifest refractions are obtained after topography, tomography, and wavefront diagnostics are performed. Instead of a cycloplegic examination, we use the Centervue DRSplus Fundus Imaging System (Icare) for the retinal evaluation in the majority of patients (Figure 14), but we will perform cycloplegia for patients with more than -8.00 D myopia, those with mixed astigmatism, and those with hyperopia. A prospective study we conducted found that these changes produced no statistical difference in our results (Figure 15).2

Figure 14. A retinal evaluation (A) performed with the Centervue DRSplus Fundus Imaging System (B) may be performed without dilation.
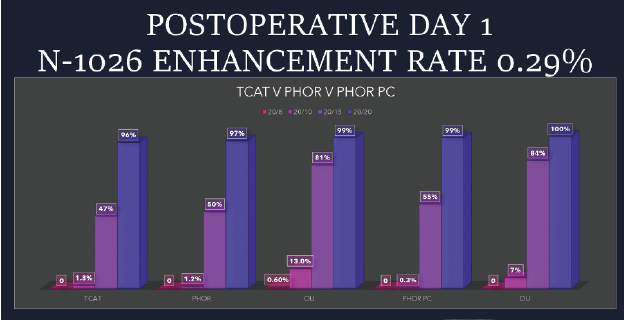
Figure 15. Enhancement rates for patients who had undergone topography-guided LASIK with new analytic software versus manifest refraction parameters.
The 1-week and 1-month postoperative visits are conducted as telehealth appointments. At the 3-month visit, a complete examination is performed for nomogram maintenance.
REFRACTIVE CATARACT SURGERY
All patients are treated as if they have selected a premium-channel package, and I explain to them how I would proceed if they were members of my family. A patient care coordinator then breaks down the pricing models for them. More than 80% of my patients choose a premium channel, whether that includes the use of a femtosecond laser, the Ocular Response Analyzer (Reichert), or premium IOLs.3,4
All patients are evaluated with OCT of the optic nerve and retina, biometry, wavefront analysis, and topography—before seeing me—and animations are used to educate them about the process and their options.5 All of this diagnostic information is entered into an EMR system and shown to patients during their examination. We use the CheckedUp Patient Engagement Platform (CheckedUp) to educate patients, and we provide them with QR codes so that they can access the information remotely to discuss with their families.
I follow lens power guidelines developed by Jack Holladay, MD, MSEE, FACS, and Warren E. Hill, MD, FACS (scan the QR codes now for related videos), and attribute my successful outcomes to them. My staff and I scrutinize angles alpha and kappa, keratometric standard deviations, root mean square higher-order aberrations, and corneal surface irregularities. Patients who have an irregular corneal surface are not offered an extended depth of focus or trifocal IOL. I personalize my lens constants and use the fourth-generation IOL power calculation formulas developed by Graham D. Barrett, MB BCh SAf, FRACO, FRACS, Dr. Hill, and Dr. Holladay for all patients. Residual refractive errors and postoperative OSD are treated aggressively.
Patients generally see well as soon as 1 hour after surgery (Figure 16). My current enhancement rate for the premium IOL channel is 1.6%. Data collection is an important part of my refractive cataract practice.6
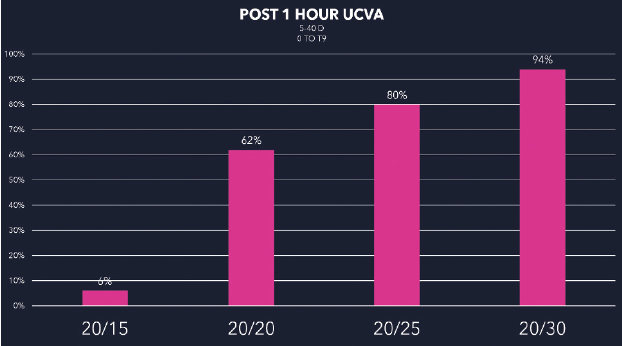
Figure 16. Postoperative single-eye UCVA 1 hour after premium refractive cataract surgery.
Figures 14-16 courtesy of Karl G. Stoneciper, MD
1. Trattler WB, Majmudar PA, Donnenfeld ED, McDonald MB, Stonecipher, KG, Goldberg DF. The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017;11:1423-1430.
2. Stonecipher KG. Outcomes of planning topography-guided LASIK with new analytic software vs. planning with manifest refraction in eyes with topography-guided parameters. Poster presented at: AAO 2020 Virtual; November 13-15, 2020.
3. Donaldson KE, Braga-Mele R, Cabot F, et al; ASCRS Refractive Cataract Surgery Subcommittee. Femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2013;39:1753-1763.
4. Stonecipher K, Parrish J, Stonecipher M, Maxwell J, Maxwell D. Femtosecond laser cataract surgery: What makes it worth it? Or not? J Ophthalmic Science. 2019;2(1):16-22.
5. Donaldson K, Fernandez-Vega-Cueto L, Davidson R, et al. Perioperative assessment for refractive cataract surgery. J Cataract Refract Surg. 2018;44(5):642-653.
6. Kieval JZ, Al-Hashimi S, Davidson RS, et al. Prevention and management of refractive prediction errors following cataract surgery. J Cataract Refract Surg. 2020;46(8):1189-1197.

