The Eye Institute of West Florida (EIWF; Figure 1) is a comprehensive multidisciplinary practice with three locations. The professional staff consists of 12 surgeons, including subspecialists in refractive surgery and cornea, glaucoma, retina, and oculoplastics; three general ophthalmologists; 11 optometrists; and one physician assistant (PA)—that’s me.
PAs are currently underutilized in ophthalmology, but we are versatile professionals who have been educated with a collaborative mindset toward medical care. This makes us suited to provide preventive care and other services in all kinds of settings, from primary care to surgery. Under the Patient Protection and Affordable Care Act, Congress recognized PAs as one of three health care professions in primary care.1 Because of our background in general medicine, PAs are flexible, and they can be responsive to changing health care needs and trends.

Figure 1. Surgical procedures are performed at the main EIWF practice location in Largo, Florida, in a state-of-the-art ambulatory surgery center on the second floor.
From a reimbursement standpoint, PAs are valuable, too. Almost all private insurers pay for PA services, and Medicare pays 85% of the physician fee schedule for services provided by the PA—and 100% if the service can be billed under incident to provisions.2
LEARNING ON THE JOB
I joined EIWF in 2012 with a background in emergency medicine and orthopedics and a strong desire to learn everything about the eye. In PA school, due to the condensed nature of the curriculum, minimal emphasis is placed on the eye, but the physicians at the practice invested in me, providing a yearlong residency-type fellowship. My training in ophthalmology involved first observing eye examinations, then learning how to do them, and finally performing them. Additionally, I observed cataract, cornea, glaucoma, retina, and oculoplastic surgeries.
My focus at EIWF includes assisting in surgeries, seeing postoperative patients, performing in-house preoperative histories and physicals, and staffing an ocular surface clinic. Assisting in glaucoma, vitreoretinal (Figure 2), and selected oculoplastic surgeries provides an extra set of hands for the surgeon, but it also benefits the practice because the PA provides reimbursable services. Surgeries at which I have assisted include trabeculectomy, implantation of an aqueous drainage device, vitrectomy, repair of retinal detachment, and dacryocystorhinostomy.

Figure 2. Ms. Crevello (left) assists Richard J. Hairston, MD, in vitreoretinal surgery.
I also help to maximize provider utilization by performing hospital consults for on-call physicians and by initiating treatments for hordeola or complex corneal conditions before referring the patient to the appropriate specialist.
Performing in-house preoperative histories and physicals provides a convenience to patients who may not be able to attend their primary care physician’s office in a timely manner before surgery. The history and physical are performed at the same appointment where the patient undergoes necessary preoperative measurements and a meeting with the surgical counselor. During this visit, I can educate patients and reassure them about their upcoming surgery. This might include answering questions about the procedure that they didn’t think to ask when they met with the surgeon and informing them about what to expect before surgery and during the postoperative period.
Source: Lane S. An eye to the future: PAs in ophthalmology. American Academy of PAs website. https://www.aapa.org/news-central/2017/06/an-eye-to-thefuture/. Accessed June 15, 2018.
DRY EYE CENTER
The EIWF is also a Dry Eye Center of Excellence, and that is where I spend the remainder of my day. It is not uncommon to hear patients state that they have been to three or more providers with their dry eye complaints before coming to the EIWF. My schedule allows me to spend precious chair time with patients, which is crucial for the management of dry eye disease. Patients are typically scheduled at 20-minute intervals, during which I perform an examination (Figure 3), do any necessary testing, and discuss treatment strategies with each patient. I take the time to listen, validate complaints, and manage patient expectations about the disease process and what to expect from treatment and management going forward. Patients feel relieved that a provider has listened and expressed optimism that relief is possible. The EIWF also has a Dry Eye Center of Excellence retail shop located in the lobby, where patients can purchase products related to their disease.

Figure 3. Ms. Crevello performs a slit-lamp examination on a patient with dry eye.
FLEXIBILITY IS THE TICKET
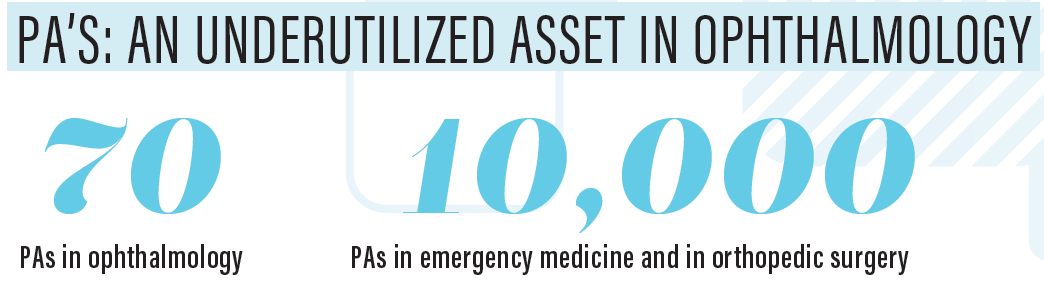
According to a publication from the American Academy of PAs (AAPA), PAs are currently underutilized in ophthalmology: In 2015, there were only about 70 PAs working in the field of ophthalmology.2 This compares with 10,000 PAs working in emergency medicine and 10,000 in orthopedic surgery.
Contrary to what may be believed, however, there are minimal, if any, regulatory barriers to PAs practicing in the eye care field. On the whole, state laws do not prevent PAs from working in the specialty, although there may be laws in some states prohibiting PAs from performing refractions.2
My flexibility as a PA has been key to boosting practice efficiency at EIWF, and the same can potentially be true of a PA at your practice, too. We can assist in surgery, evaluate and treat patients in the clinic, see postoperative patients, and perform hospital consults, and this versatility is what makes us so valuable in a busy, high-volume multispecialty practice.
1. Employing a PA. American Academy of PAs website. https://www.aapa.org/career-central/employer-tools/employing-a-pa/. Accessed June 15, 2018.
2. Lane S. An eye to the future: PAs in ophthalmology. American Academy of PAs website. https://www.aapa.org/news-central/2017/06/an-eye-to-the-future/. Accessed June 15, 2018.