


Performing an IOL exchange in the presence of an open posterior capsule presents both a challenge and an opportunity. A frequent challenge in these eyes is having to manage the vitreous. Opportunity arises from access to the middle and posterior segments without having to go through the pars plana. As when the posterior capsule ruptures during cataract surgery, a vitrector can be inserted into this critical space to debulk the vitreous and prevent it from coming forward.
ONE-PIECE IOLS
Assuming the IOL–capsular bag complex is stable, I forgo a pars plana approach and dissect the anterior capsule off the IOL. Next, I typically attempt to sneak an OVD cannula around the IOL and tamponade any vitreous backward away from the lens. I then carefully work to remove the haptics of the one-piece IOL. Explanting them is less important to me in this situation because the replacement IOL will not be implanted in the bag. My threshold for amputating the haptics and removing only the optic is therefore quite low. This strategy helps prevent undue strain on the bag complex and preserve the sulcus as a safe zone with plenty of support for a new IOL. Once the optic is in the anterior chamber, the process for its removal is the same as if the capsule were intact with the caveat that motions inside the eye should be especially gentle to prevent vitreous from coming forward.
After optic removal, IOL exchange surgery proceeds similarly to if the posterior capsule had ruptured. A thorough anterior vitrectomy is performed by placing the vitrector in the anterior vitreous. It can be tempting to sweep the instrument back and forth, but keeping the vitrector in one place is the best way to prevent traction. Once a thorough anterior vitrectomy has been performed, the space is filled with a dispersive OVD, and the irrigation cannula is removed.
My lens of choice for these eyes is a hydrophobic three-piece such as the Tecnis aspheric monofocal (model ZA9003; Johnson & Johnson Vision). If the anterior capsule is not overly fibrotic, then the optic is captured posterior to the anterior capsule, and the PMMA haptics are left in the sulcus. If I suspect that the IOL may fall or that manipulating the IOL-bag complex could damage the zonules, then I perform an anterior vitrectomy through the pars plana before addressing the IOL.
THREE-PIECE IOLS
For the purposes of this discussion, I am presenting the following scenario: A patient who had cataract surgery 15 years ago develops calcification of a silicone three-piece IOL after undergoing an Nd:YAG laser capsulotomy (Figures 1 and 2). The lens design is advantageous because thin PMMA or PVDF haptics are much easier to remove from a fibrotic capsule than those of a one-piece IOL.

Figure 1. A calcified silicone IOL.
Figures 1 and 2 courtesy of J. Morgan Micheletti, MD
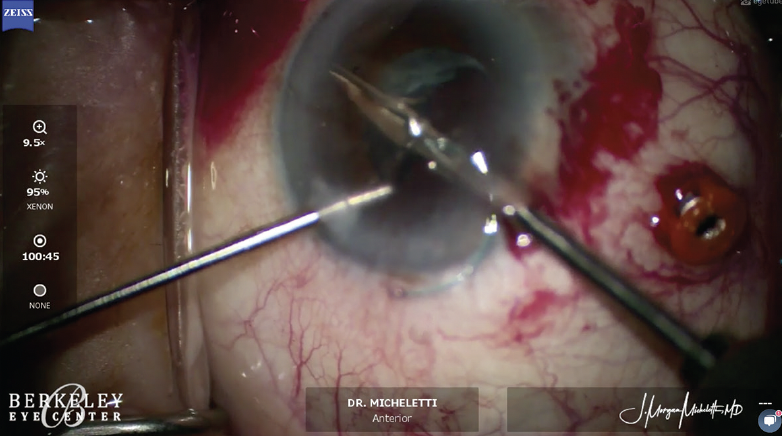
Figure 2. Patience is required when cutting the optic of a silicone IOL.
My approach in this situation would be the same as I described earlier, but I would be more confident that I could remove the entire IOL instead of leaving the haptics behind. The challenge with a silicone lens is that grasping and manipulating the optic is harder than grabbing and moving a greased watermelon. It is therefore difficult to cut the optic and remove it through a small incision. Patience when cutting the lens—sometimes into multiple pieces—is key.
After removal of the optic, a thorough vitrectomy would be performed through the open posterior capsule, a three-piece hydrophobic acrylic IOL would be implanted in the sulcus, and the optic would be captured. (See below for a video demonstration of IOL exchange of a calcified silicone IOL performed by J. Morgan Micheletti, MD.)
Some surgeons place the new IOL scaffold under the old IOL before explanting the original lens. This can be an effective strategy. I, however, feel obliged to perform an anterior vitrectomy first because it runs the risk of incarcerating vitreous around the new IOL as it is implanted.

