





Intrastromal corneal ring segments (ICRSs) are used mainly to reduce myopia and astigmatism in patients with keratoconus. ICRS erosion, either inward or outward, is a rare but severe complication. Typically, exposure is external, and the ICRS protrudes through the corneal epithelium. Patients often experience an intense foreign body sensation, and the area surrounding the exposed ICRS fluoresces. Anterior segment OCT (AS-OCT) imaging is seldom required, and segment removal is usually necessary.
Less frequently, as in this case, ICRSs erode through the Descemet membrane and into the anterior chamber. Patients present with symptoms similar to those of individuals with hydrops—pain, redness, and photophobia.
THE CHALLENGE OF ACCURATELY IDENTIFYING ICRS EROSION
AS-OCT imaging can be useful for visualizing the position of the ICRS because the slit-lamp view is likely to be clouded by edema. The high reflectivity of the segment’s PMMA material, however, can introduce artifact. Figure 1 demonstrates ICRS erosion into the anterior chamber. Only reflections of the edges of the segment are visible because reflectivity within the segment itself is minimal. Additionally, a tight, white wishbone of Descemet membrane surrounds the portion of the ICRS that has invaded the anterior chamber.
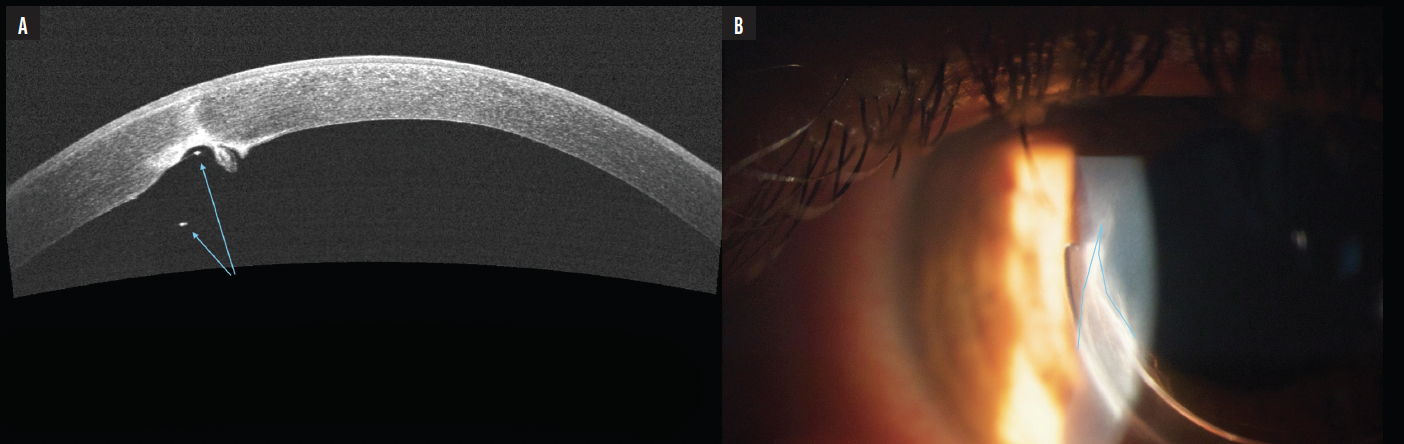
Figure 1. An AS-OCT image shows ICRS erosion into the anterior chamber (A). The blue arrows indicate reflections from the ICRS edges, and a rounded flap of Descemet membrane is visible. A slit-lamp examination reveals a wishbone-shaped Descemet tear (blue outline) caused by the internal erosion (B).
Reflection artifacts on AS-OCT imaging occasionally prompt the misidentification of internal erosion when, in fact, the ICRS is appropriately positioned. Unlike with an eroded ICRS, reflection artifacts appear as well-organized tissue layers in a nonanatomic position posterior to the surrounding cornea (Figure 2). A slit-lamp examination, moreover, does not reveal edema or abnormalities in the Descemet membrane.
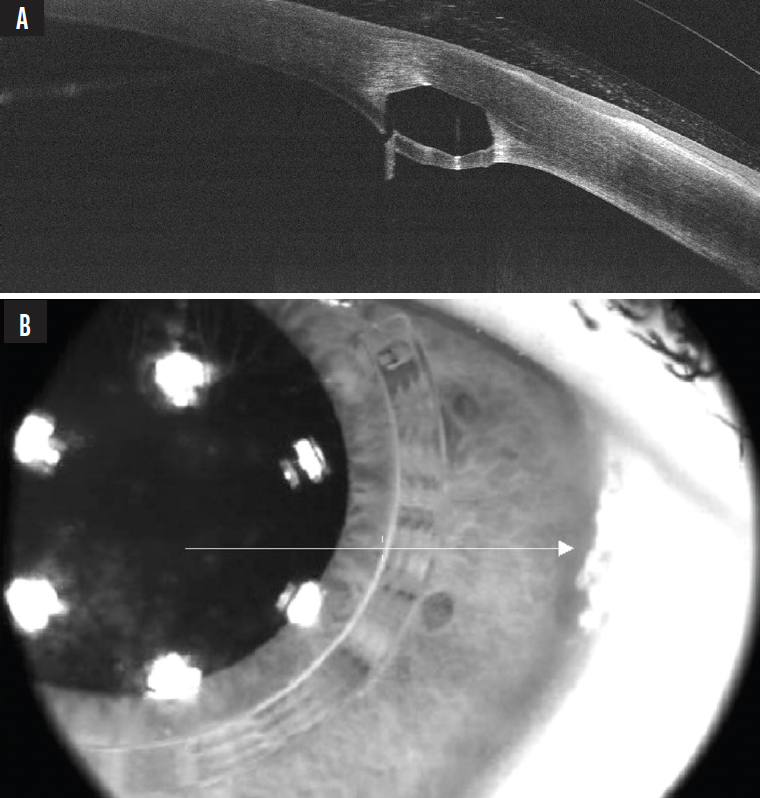
Figure 2. AS-OCT image of the ICRS showing artifactual reflections despite no actual erosion through the Descemet membrane (A). No associated edema or other abnormalities are visible at the slit lamp or in an infrared image (B).
SURGICAL PEARLS
When removing an ICRS that has eroded through the Descemet membrane and entered the anterior chamber, it is important to preplace a paracentesis for anterior chamber access in case of expected chamber collapse. Aqueous egress through the tunnel is likely to cause the chamber to flatten upon ICRS removal. To stabilize the chamber, filling the tunnel with air can create a surface tension tamponade. Additionally, placing a suture is likely necessary due to the chronic stretching of the stromal tunnel.

