




The double-needle, sutureless intrascleral haptic fixation (ISHF) technique was originally described by Yamane et al in 2017.1 The technique’s advantages include a small incision, short operating time, and lower risk of postoperative hypotony compared to larger-incision scleral fixation techniques. This technique, however, is associated with a steep learning curve to avoid tilt and decentration. A wave of a modified intrascleral fixation techniques have subsequently been described.2,3 Identifying when adjustment is necessary can result in a safer outcome. This article shares our suggestions and observations to help surgeons in search of the perfect fixation technique.
SETTING UP FOR SUCCESS
The double-flanged ISHF technique is an elegant approach to secondary IOL fixation. The best IOLs for ISHF are the CT Lucia 602 (Carl Zeiss Meditec) and Tecnis monofocal three-piece (model ZA9003 or AR40e, Johnson & Johnson Vision). Ideal materials include 30-gauge thin wall needles (TSK) on a tuberculin syringe filled with balanced salt solution, Duet forceps (MicroSurgical Technology), low-temperature cautery to create the flanged haptic, and infusion. Infusion can be accomplished through an anterior chamber maintainer or pars plana trocar. Most importantly, a thorough pars plana–assisted or limbus-based anterior vitrectomy should be performed before or concomitant with surgery. Fortunately, many patients requiring this procedure have already had a pars plana vitrectomy that adds to the safety of the implantation maneuvers.
Reproducibility improves the likelihood of achieving safe and predictable outcomes. Yamane et al described the steps for attaining optimal outcomes.1,4 These include placing marks at 180º for X/Y centration, directing the scleral tunnel at a 15º to 20º angle toward the limbus, using a 5º posterior entry to avoid deformation of the haptics, and entering the eye 2 to 2.5 mm posterior to the limbus depending on the white-to-white distance (Figure 1; Video). The steps of the procedure are described in The Technique in Detail. Standardization of the ISHF technique, however, is challenging in the setting of conjunctival chemosis and inevitable variations in tunnel length and entry. Markers have come to market that attempt to address some of these issues.
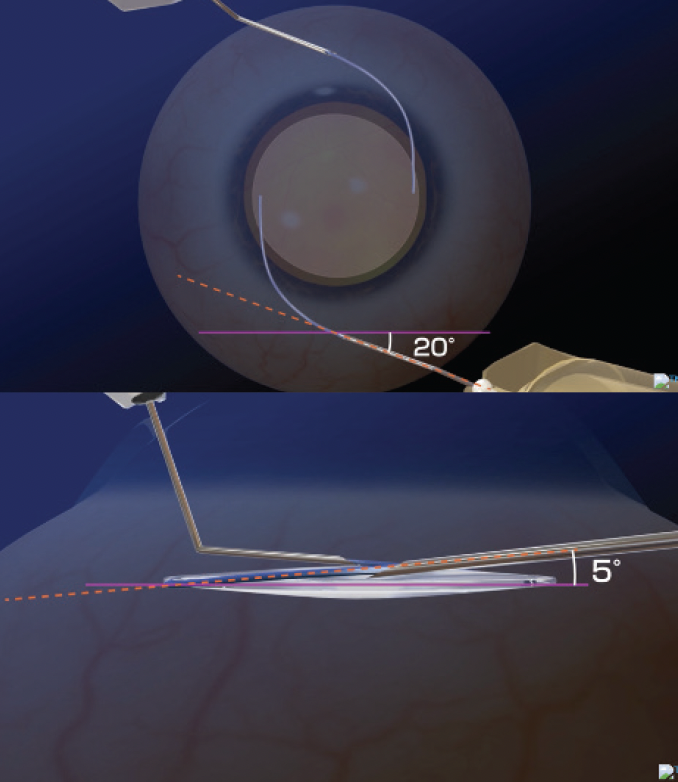
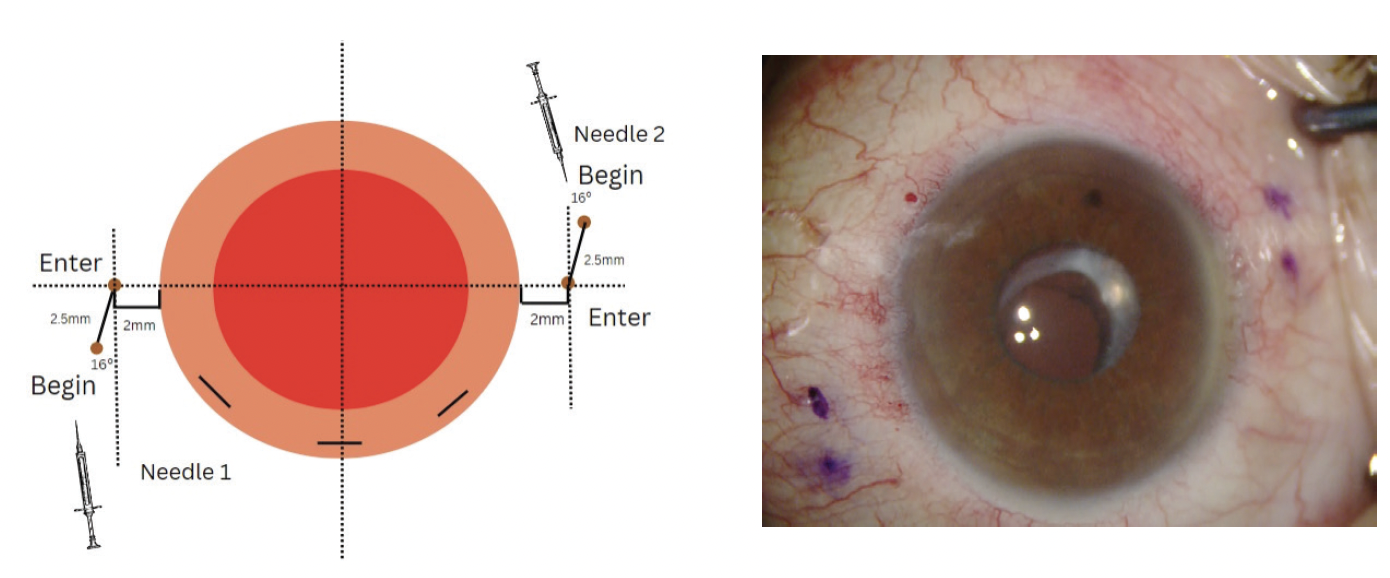
Figure 1. A schematic of the entry wound 2 mm posterior to the limbus, a 20º tunnel entry to the limbus, and a 5-mm posterior angulation of the sclerotomy.
Figure 1 courtesy of Shin Yamane, MD, ASCRS Film Festival Video (2016)
Proper anesthesia is important to success. A retrobulbar or sub-Tenon block is preferred because scleral tunnels are involved. Many have recommended choosing a refractive target of -0.50 to 0.75 D to achieve emmetropia.5
COMPLICATIONS AND INTERVENTION
ISHF remains a two-point fixation technique that can result in IOL tilt, decentration, and pupillary capture. Ignoring these issues both during and after surgery can lead to pigment dispersion, uveitis-glaucoma-hyphema syndrome, iris and transillumination defects, cystoid macular edema, and an undesirable refractive outcome.
Pupillary capture. Careful marking can help prevent pupillary capture, which is typically caused by optic tilt or severe iridodonesis (Figure 2). Superior pannus, however, can make marking the eye difficult. At a minimum, the surgeon should look for the dirty limbus, (the portion of the cornea that is covered by pannus) and measure from where it meets the sclera. When in doubt, the conjunctiva can be taken down to identify the termination of the blue zone and the eye entered 1.5 mm posterior to this point. If there is obvious tilt with pupillary capture intraoperatively, the haptic closest to the side of the optic that is captured should be redocked 1 mm more posteriorly. After repositioning, it can be helpful to instill intracameral miotics to test the eye’s propensity for pupillary capture. An intraoperative surgical peripheral iridectomy can promote equilibrium in anterior and posterior chamber fluidics and thereby decrease the likelihood of postoperative pupillary capture. (For tips on pupillary capture, watch the video below.)
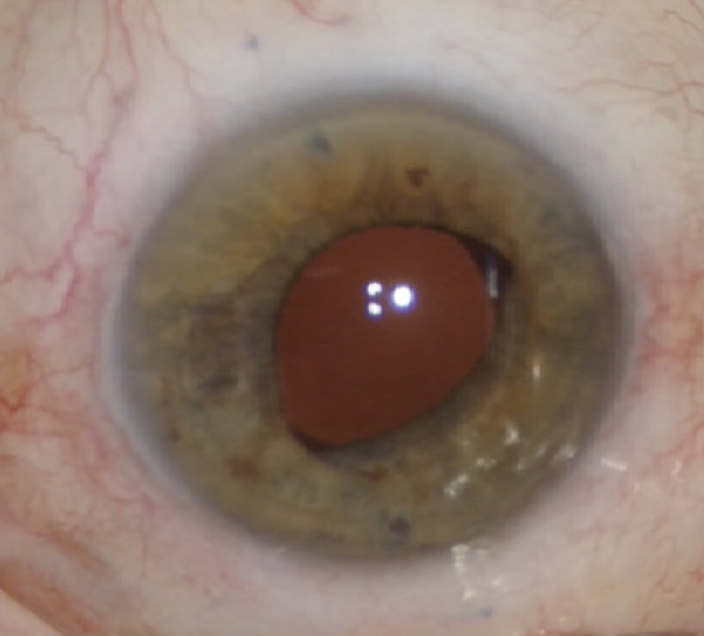
Figure 2. Pupillary capture despite two laser peripheral iridotomies in the office. The arrow designates the haptic to be repositioned more posteriorly.
When postoperative pupillary capture occurs, ultrasound biomicroscopy is critical to determining whether the IOL is tilted and requires repositioning or iridodonesis is present. In some instances, dilating and then slowly bringing down the pupil with miotics may release the optic. In eyes with severe iridodonesis, one or two laser peripheral iridotomies may be performed.6 The goal is to address the underlying issue to avoid chronic inflammation, iris damage resulting in intractable glare, and uveitis-glaucoma-hyphema syndrome.
IOL decentration. Mild superior or inferior decentration may be resolved by shortening and reflanging one haptic with low-temperature cautery (Figure 3). If decentration is severe and too far nasal or temporal, the eye should be re-marked at 180º and the haptic should be redocked for better centration.
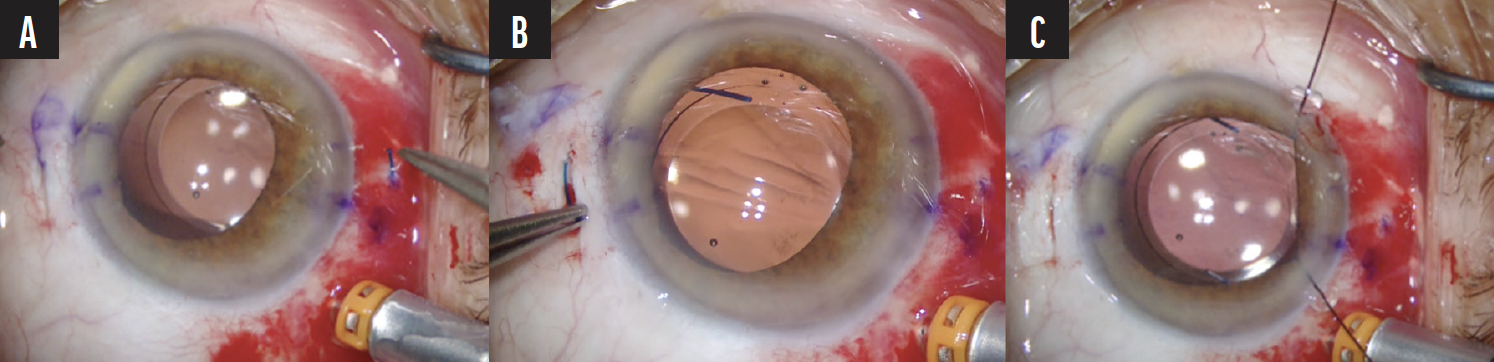
Figure 3. Decentered IOL due to slight asymmetric tunnel length (A). The haptics are shortened no more than 1.5 mm and reflanged with low-temperature cautery (B). Recentration is confirmed with iris hooks (C).
IOL tilt. Typical causes of tilt are asymmetric needle entry from the limbus and asymmetric tunnel length (Figure 4). Reproducible tunnel length and entry are challenges with the Yamane technique. When significant intraoperative tilt is observed, the side dipping posteriorly likely has a shorter tunnel. The flange, if already made with cautery, can be cut on a bevel and tested outside the eye with a 30-gauge thin wall needle. The haptic is then reinserted into the eye and placed on the iris. The new tested 30-gauge thin wall needle can then be redocked for a longer tunnel and properly placed from the limbus. An IOL with polyvinylidene fluoride haptics is useful for redocking because they resist kinking better than PMMA haptics.
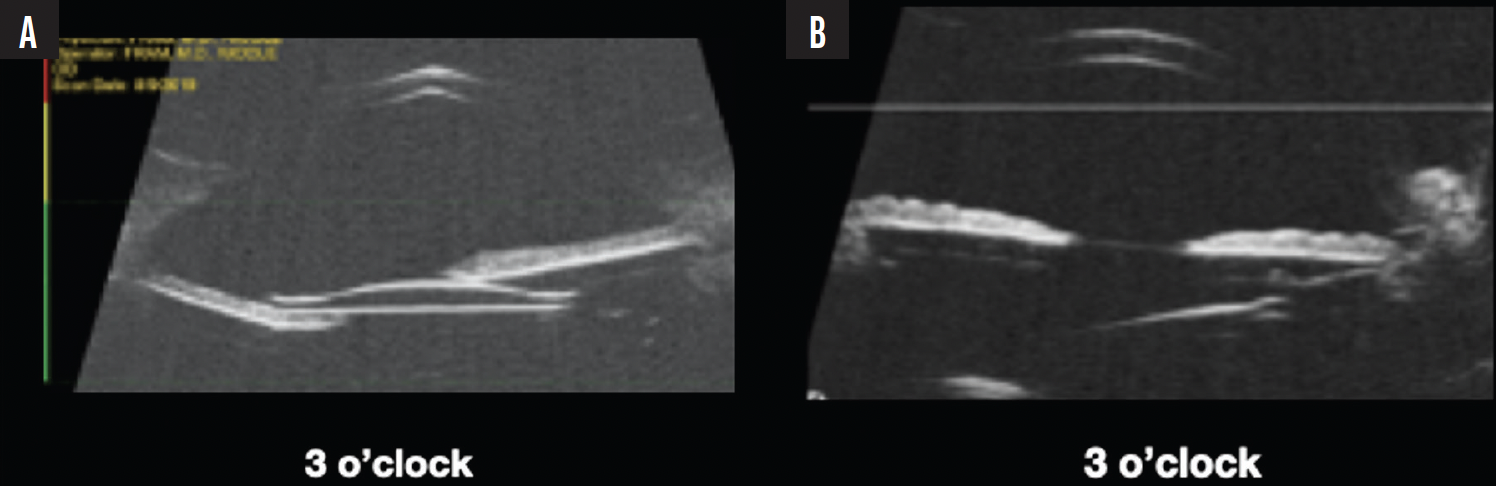
Figure 4. Ultrasound biomicroscopy of two patients. UBM confirmed that IOL is not tilted, and there is severe iridodonesis necessitating peripheral iridotomies with or without pupillary cerclage (A). UBM confirmed that the IOL is tilted and requires refixation to prevent chronic iris chafing and UGH (B).
Extruded and kinked haptics. Postoperatively, in the event that a haptic has extruded through the conjunctiva and been exposed to the ocular surface with keratin, bacteria, and conjunctival flora, reimplantation can lead to infection. If significant scleritis surrounds the extruded flange, a patch graft can be attempted, but it rarely solves the underlying issue. If inflammation underneath the patch persists, chronic iritis and cystoid macular edema may result (Figure 5). In many cases, it is best to remove and replace the IOL entirely.
Figure 5. An extruded flange and haptic with keratization that were missed for 1 year caused chronic recalcitrant cystoid macular edema.
THE TECHNIQUE IN DETAIL
Marking. The figures at left detail the markings required for the intrascleral haptic fixation technique. Initial marks are made 2 to 2.5 mm posterior to the limbus and 180º apart. An additional 2.5-mm mark is made in a counterclockwise fashion. The marks can be made freehand with calipers or any of several commercially available devices such as the Fram Marker (Epsilon), Yamane marker (Geuder), or Kim calipers (Epsilon). An angled scleral tunnel is created at a 15º to 20º angle to the limbus to follow the natural path of the peripheral haptics and limit stress on the haptics.1 The more posterior the sclerotomy entry, the greater the likelihood that the IOL-haptic complex will be on stretch, increasing the potential for tilt. Careful measurements are crucial.

Incisions. A central 3-mm main incision and two 1-mm adjacent paracentesis incisions are created (yellow lines in figure). An anterior chamber maintainer is placed. A trocar is placed if an additional procedure such as an IOL exchange (see video below) or pars plana–assisted anterior vitrectomy is planned. It is helpful if the main incision is located at least 110º from the trailing haptic sclerotomy to facilitate docking of the trailing haptic.
Needle Preparation. As described by Sumit “Sam” Garg, MD,2 the needles are prepared and marked 1 and 2. The first needle is bent bevel up, and the second needle is bent bevel to the left.
First scleral tunnel. The first scleral tunnel, created with needle 1, begins at the first mark and extends to the second mark. The needle is turned to enter the eye. In the original technique, the needle is removed from the syringe and left in the tunnel. We prefer to move directly to lens insertion. Judging the depth and length of the scleral tunnel can be challenging for those new to intrascleral haptic fixation. If the tunnel is too superficial, tilt and haptic erosion are likely because the bulb sits near the Tenon space. If the tunnel is too deep, it will be short as the eye is entered prematurely. The needle should not be visible as it passes within the sclera; if the needle is visible, it is too superficial. A 15º angle of approach prevents too deep an entry until the final pivot is performed. These adjustments can be made with repeat passes if necessary.

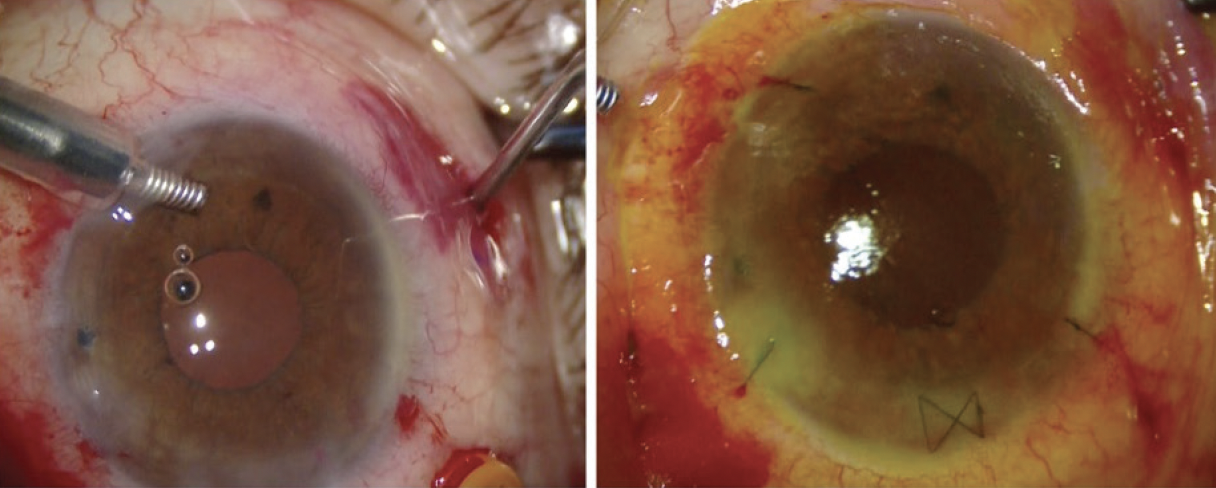
Peripheral iridotomy. A peripheral iridotomy is performed with the vitrector. We recommend using I/A cut mode with a high vacuum level and a low cut rate.
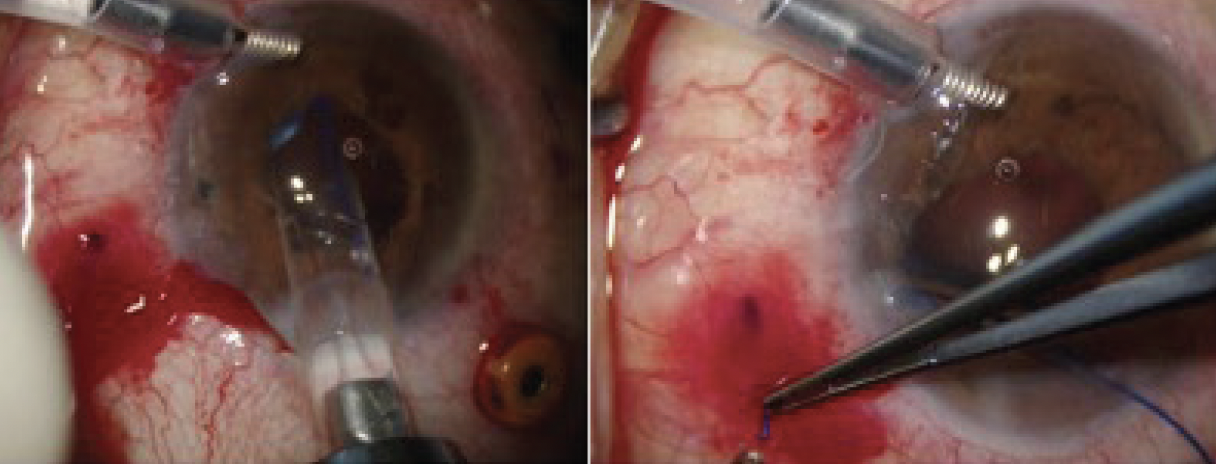
Conclusion of the surgery. The haptics are tucked within the scleral tunnel by pushing them gently with the end of a cannula (figure at left). At the end of the case, the haptics are buried, the wounds are sutured (figure at right), and the lens is centered.
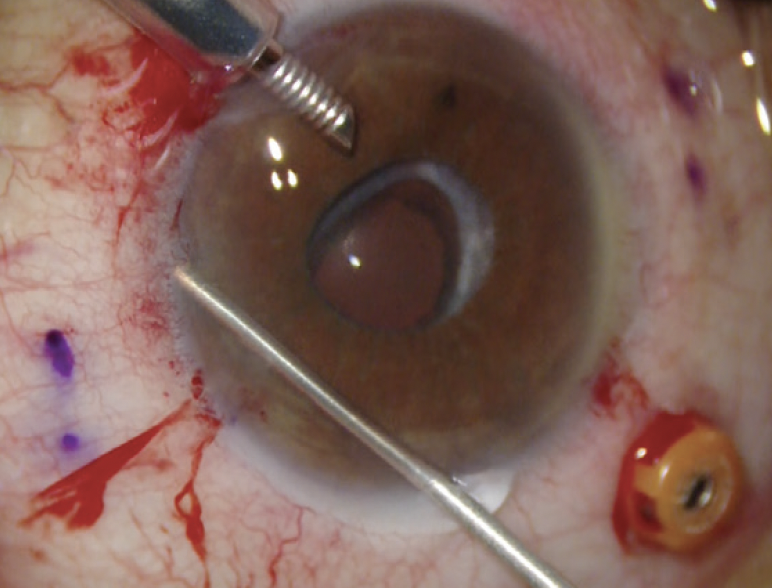
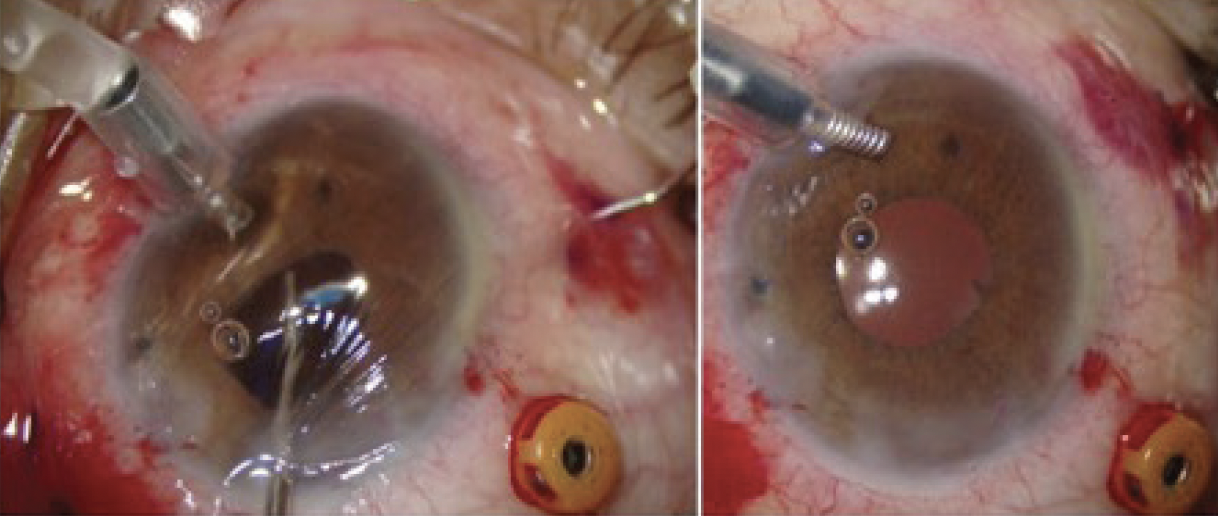
Haptic 1. The IOL is injected into the anterior chamber (figure at left). Forceps are used to insert the haptics into a 30-gauge thin wall needle (TSK). A modification described by D. Brian Kim, MD, is to inject the lens directly into the anterior chamber and dock the haptic into the first needle in one motion.3 This technique requires a technician to assist by turning the plunger to inject the lens. Once the haptic is in the needle bore, the first needle can be removed and the haptic cauterized to a bulb (figure at right) or left docked in the 30-gauge thin wall needle depending on the surgeon’s preference.
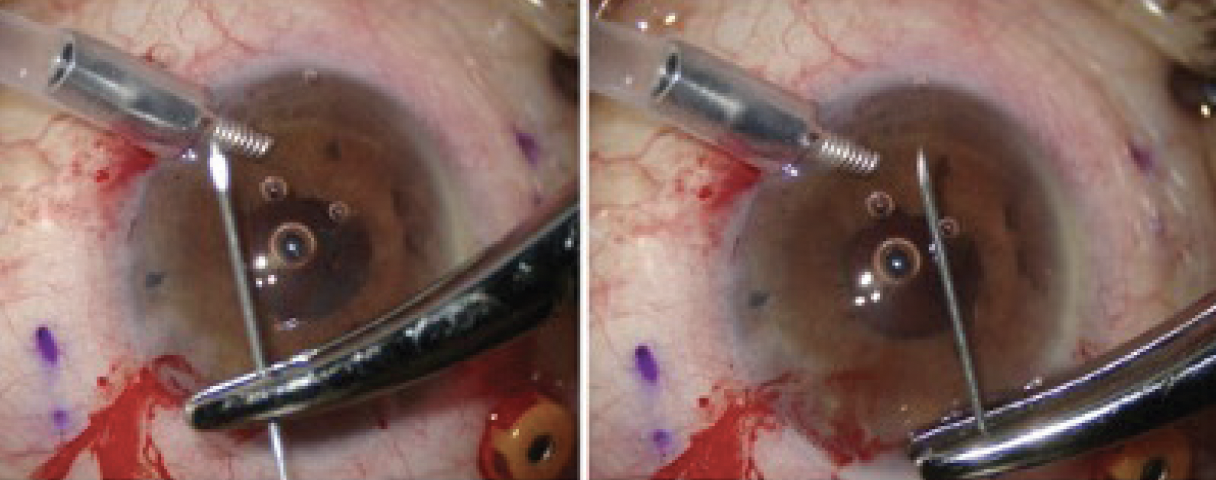
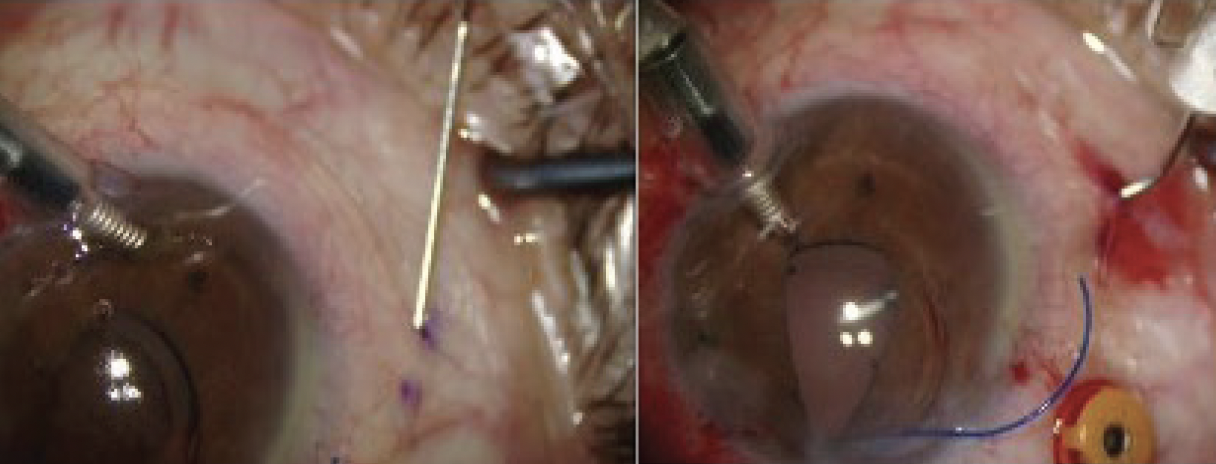
Scleral tunnel 2. The scleral tunnel, created with needle 2, begins at the opposite first marking and extends to the second marking (figure at left). The needle is turned to enter the eye at exactly 180º from the previous entry (figure at right).
Haptic 2. The most challenging part of the technique is inserting the trailing haptic into the second needle. Considerations include holding the haptic 2 mm from the tip, orienting the needle to provide a backboard to enter, and carefully removing the second needle in a controlled fashion. A second haptic bulb is created using low-temperature cautery. If the surgeon’s preference is to leave the trailing haptic outside the incision before docking, the main incision should be located at least 110º away from the sclerotomy to simplify docking.
1. Yamane S. Transconjunctival intrascleral IOL fixation with double-needle technique. Video presented at: ASCRS/ASOA Annual Meeting; May 6-10, 2016; New Orleans.
2. Garg S. Common intraoperative mistakes of the beginner and how to avoid them. Paper presented at: 2020 ASCRS/ASOA Virtual Annual Meeting; May 2020.
3. Kim DB. The next big thing in scleral haptic fixation. Cataract & Refractive Surgery Today. October 2017;18(10):27-36.
1. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136-1142.
2. Rocke JR, McGuinness MB, Atkins WK, et al. Refractive outcomes of the Yamane flanged intrascleral haptic fixation technique. Ophthalmology. 2020;127(10):1429-1431.
3. Canabrava S, Andrade N Jr, Henriques PR. Scleral fixation of a 4-eyelet foldable intraocular lens in patients with aphakia using a 4-flanged technique. J Cataract Refract Surg. 2021;47(2):265-269.
4. Yamane S. Transconjunctival intrascleral IOL fixation with double-needle technique. Video presented at the: ASCRS/ASOA Annual Meeting; May 6-10, 2016; New Orleans.
5. McMillin J, Wang L, Wang MY, et al. Accuracy of intraocular lens calculation formulas for flanged intrascleral intraocular lens fixation with double-needle technique. J Cataract Refract Surg. 2021;47(7):855-858.
6. Singh H, Modabber M, Safran SG, Ahmed II. Laser iridotomy to treat uveitis-glaucoma-hyphema syndrome secondary to reverse pupillary block in sulcus-placed intraocular lenses: case series. J Cataract Refract Surg. 2015;41(10):2215-2223.

