With the many advances in diagnostics, IOL designs, and surgical technologies in recent years, ophthalmologists today have an unprecedented opportunity to offer cataract surgery patients the kind of refractive accuracy that used to be the domain of only the refractive surgeon. Whether through astigmatism correction, multifocality or blended vision, aspheric lens technologies, or some combination of these, we can provide cataract patients with clear vision at a range of distances.
But this capability comes with a price. First, there is the cost of the technologies, including advanced diagnostic equipment for biometry, keratometry, and topography, and surgical equipment possibly including a femtosecond laser, intraoperative aberrometry and OCT, and other devices.
More important, however, is that you want to provide a premium experience to the patient, who is paying a premium price for a premium IOL. This likely means making changes to the office setting and to the way patient visits are structured. Faced with these hurdles, what does the established comprehensive ophthalmologist need to do to begin offering refractive cataract surgery? Having been through the process myself, I have some ideas on the subject, and several suggestions are presented in this article.
FIRST, COMMIT
Probably the first and most important step for the comprehensive ophthalmologist who wishes to enter the field of refractive cataract surgery is to commit to the change. There’s no question that change starts at the top, and, if the surgeon is not fully invested in the process, the staff certainly won’t be. Once the practice leader is committed to this new direction—once he or she understands and believes in the technology needed to achieve excellent quality of vision—the process of change can begin.
Equally important is the second step, which is for the surgeon to get the staff on board and committed to the change. This is vital to everything that comes after. From this point forward, there will be a lot of work to be done, and much of it will fall to the staff—from the front desk, to the technicians, to the back office. It will be important, for example, to determine how to explain premium IOLs in lay people’s language, so that patients will understand the options that are being offered to them. All staff members then must learn the language and become fluent with it. The doctor and staff need to work together on this, so that ideas can be presented to patients in a simple and straightforward fashion and in language that is shared by everyone in the practice.
PRESENTING OPTIONS
Once you are sure you have staff buy-in, you and your staff must work out the details of the patient encounter. How and when will information be presented to patients? Who will present the information? And how do you ensure that patients understand their options? As these decisions are made, the contours of the patient experience will begin to take shape.
How and when is information presented? Some options include sending out information to the patient when the consultation appointment is made, directing patients to a website (Figure 1), and presenting the information during the initial visit.
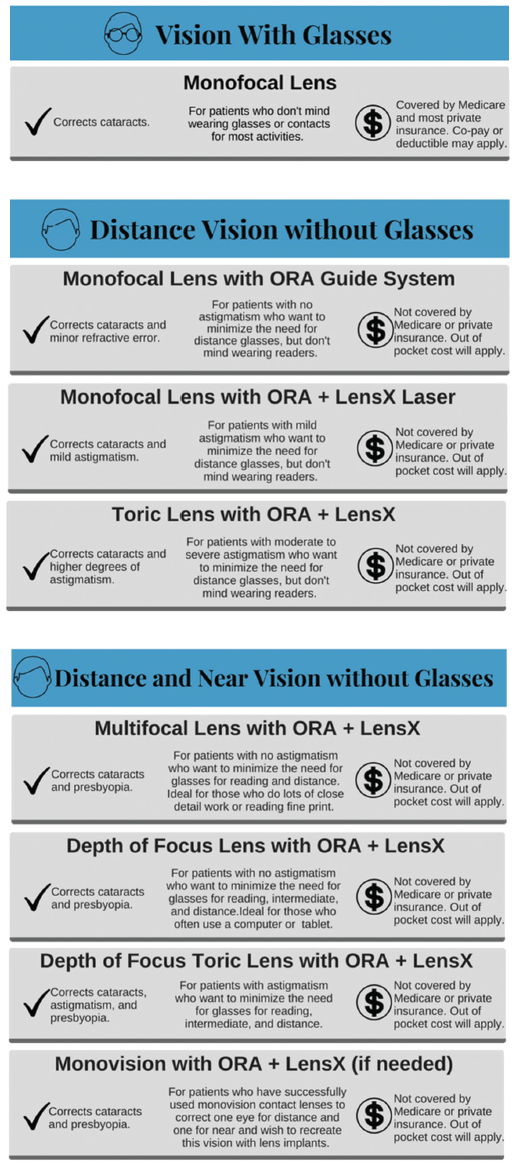
Figure 1. Dr. Solomon’s personal website (www.drkerrysolomon.com) includes information for patient education, including lens options broken down by lifestyle needs.
Who will present the information? The first decision is to figure out if the staff will present the information to the patient during the visit, before he or she sees the doctor, or if the doctor will be the first one to present it. The second decision is to delegate who manages the closing conversation—again, the staff or the doctor.
Most doctors don’t want to be the person first presenting options to patients. They prefer for information to be presented by a counselor or an educator, and then the doctor can answer any questions that the patient still has and make a recommendation.
How do you ensure that patients understand their options? In discussions with patients, try to take cost off the table and concentrate on understanding the why: Why does this patient want to be less dependent on glasses? Once the why is understood, then cost becomes less of an issue. If the patient is motivated by a particular reason, use that information to guide the patient and find a way to make it happen with multiple options for financing.
Part of the reason for understanding the why is so that you can narrow the options presented to patients. Take the patient who says: “I really want to be able to see in the distance and up close without needing to be dependent on glasses.” Because you know what that patient wants, you do not need to waste time presenting all the options for intermediate vision, monovision, and blended vision, for instance.
If too many options are presented, there is a risk of confusing the patient and paralyzing him or her with choices. The confused patient is likely to give up. Rather, there is merit to presenting the best option in a simple way and providing a recommendation.
In the process of designing the patient experience, then, many of the patient’s desires—the why—can be determined ahead of time through a questionnaire of visual preferences, the testing performed, and the staff’s patient education. Then, when the patient finally sees the doctor, the doctor can say: “Based on what you’ve said you’re looking to achieve, and based on your exam and your testing results, I’d recommend [whatever option you’ve concluded is best].” That brings the consultation to a satisfying conclusion.
MANAGING OUTCOMES
Another aspect of offering refractive cataract surgery is managing your surgical outcomes. When you ask patients to pay a premium to be less dependent on glasses, you have to make sure you can achieve that goal.
Improving your outcomes means collecting pre- and postoperative data and either sending it to a service for analysis or obtaining software to do it yourself. For example, the web-based program Veracity Surgical (Carl Zeiss Meditec; Figure 2) uses data from your electronic health records and diagnostic devices to analyze your outcomes. With that service or another software program, you can start optimizing your outcomes, so that the likelihood of achieving your refractive target improves from a level of 60% to 70%, up to 80% or 90%.
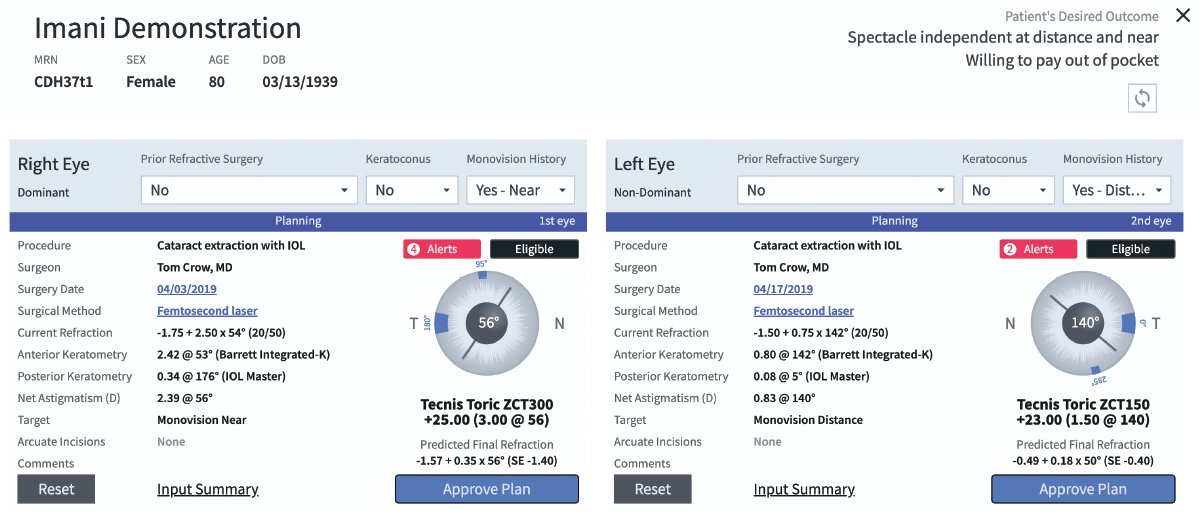
Figure 2. The web-based Zeiss Veracity Surgical platform houses patient data on a secure cloud and can be integrated with electronic health records and diagnostic devices.
Still, even if the likelihood of getting the result you want is high, you need to have enhancement strategies such as PRK or LASIK available to you. As a comprehensive ophthalmologist, if you are not set up to do corneal refractive surgical enhancements, you can arrange for someone else in your practice or someone in the community to provide that service for you.
And you should make clear to patients that any necessary enhancements are part of the package—a package that includes everything that’s been discussed. It’s helpful to tell patients that you will provide every piece of technology at your disposal to help them achieve the outcome they’re looking for.
GETTING THERE
The changes I’ve described are all vital, but there’s still more work to be done. If you’re looking to develop a refractive cataract practice, then I believe you need to have a refractive cataract mindset. Whether you decide to set up a separate space in your practice for premium patients or you want to switch your whole practice over to premium service, you have to adopt a concierge service style. There are many ways to approach it, but the result must be that patients don’t wait to be seen and they feel that their time is valued.
Make visiting your practice a positive experience. Patients are seen on time, greeted with a smile, and have their expectations set from the start: “My name is [X]. I’m going to be doing [this testing], then I’m going to hand you over to [Y] for [something else]. Your total visit should be about 2 hours. At the end, you’ll see the doctor.” Each visit should be well-orchestrated and fully choreographed, consistent from patient to patient.
Designing the visit is another process in and of itself. This is where the staff becomes a team, as everyone works out the process of how patients will be seen. If you were the patient, how would you want to be seen? Script the visit based on that notion. Do role playing. Develop time sheets to track and follow the patient’s progress over time. Monitor everything, and tweak it monthly, quarterly, and annually. It is a lot of work, but, at the end of the day, average wait times of less than 15 minutes are achievable. If patients are seen on time and their customer experience is good, they’re more open to elective options, and they have confidence that this office is capable of delivering the results described to them.
With the added work and training required, the staff should be rewarded. Some practices use bonus plans to reward staff for the right kind of behavior. In some instances, you might need to change your staff or weed out certain people. Having the right team in place is paramount.
CONCLUSION
There’s no question that setting out to provide refractive cataract surgery is a labor of love, but it’s so rewarding when you get there. There’s no question in my mind that it is a worthwhile exercise.
And, in my opinion, the modern cataract surgeon has to do it. Patients are living longer, they’re leading more active lives, and there is tremendous interest on their part in being less dependent on glasses. Lastly, it’s a rewarding way to practice. Patients are thrilled when they can not only have their vision improved after cataract surgery but, perhaps for the first time in their lives, can be less dependent on glasses.
It’s a big opportunity, and if you don’t offer it in your practice a percentage of your patients are going to seek a second opinion and go elsewhere. From a business standpoint, elective procedures can be a big portion of the income for many practices.
As noted, refractive cataract surgery requires a different mindset. Perhaps you see fewer patients, but you treat them with a higher level of customer service. It allows you to understand your patients’ needs and really work to provide the vision they’re looking for and the lifestyles that they want to lead.