



Over the past several years, our practice has noted an increased level of expectation on the part of our cataract surgery patients. Patients often state that, after surgery, they want to have not only excellent uncorrected distance vision but also good midrange and near vision. Patients are aware that there are refractive cataract surgery options, and the demand for these services has increased in almost all ophthalmic practices. This situation has created an opportunity for us to improve both patient care and the financial security of our practice.
In the past, cataract surgery was the definitive sign of old age, but now, for many, it is a potential fountain of youth. With this as a background, it is important to understand that, in the business of refractive cataract surgery, there are three basic but vital concepts:
No. 1: Recognize the demand for refractive cataract surgery;
No. 2: Be prepared to seize the opportunity; and
No. 3: Have the right solutions.
NO. 1: RECOGNIZE THE DEMAND
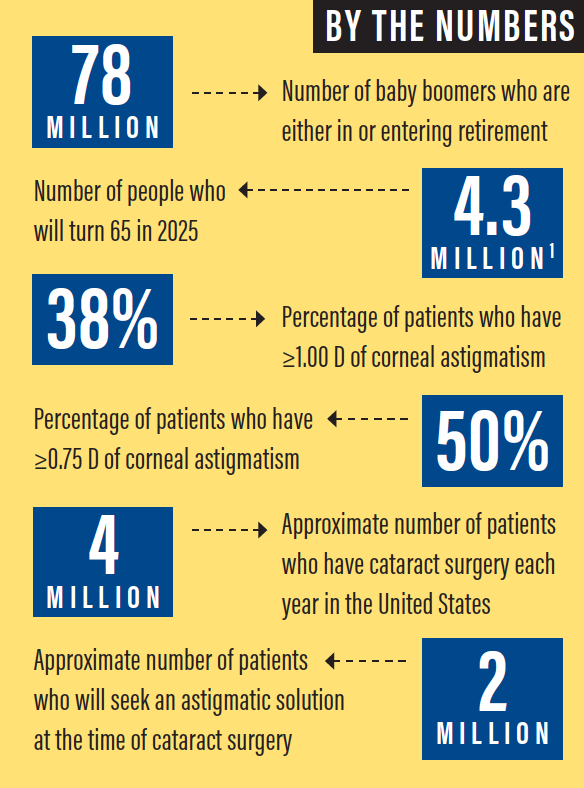
We all know that the population is aging, with 78 million baby boomers either in or entering retirement. In 2025, 4.3 million people will turn 65.1 Among patients who have the resources, there is an increased willingness to spend money for their own benefit to support a more active lifestyle. Patients are living longer, they have a desire to look and feel good, and they are willing to invest out of pocket for a significant return on investment for their health.
The opportunity for refractive cataract surgery starts with the low-hanging fruit for the refractive surgeon, and that is the reduction or elimination of astigmatism. Approximately 38% of patients have 1.00 D or more of corneal astigmatism, and approximately 50% have 0.75 D or more. All of these patients could benefit from an astigmatism-correcting toric IOL or possibly incisional astigmatic surgery.2 Almost 4 million patients a year have cataract surgery in the United States; many of them will seek a presbyopic solution, and, potentially, 2 million will seek an astigmatic solution.
The key for surgeons interested in refractive cataract surgery is accessing new technology. A variety of recently introduced technologies have improved patient outcomes, and the surgeon who wishes to offer refractive cataract surgery must be comfortable with these technologies.
No. 2: SEIZE THE OPPORTUNITY
Refractive cataract surgery is extremely important to our practice. The patient-shared billing opportunity of refractive cataract surgery reduces the impact of insurance reimbursement declines; it increases the profitability of surgery centers and laser centers; and, most important, it improves patient satisfaction, which equates to practice growth. We employ several important business principles to support this aspect of the practice. For example, access to technology for refractive cataract surgery is extremely important for patient care and practice stability. We make sure that, when we adopt a new technology, we educate all of our surgeons to improve their familiarity with and boost their adoption of this newest option.
We perform minimal external marketing, but we have extensive internal marketing through websites, brochures, posters, and social media. We also employ dedicated internal and external refractive coordinators.
For patients who experience suboptimal results, we provide refractive enhancements at no cost to the patient, and we have surgeons who can perform limbal relaxing incisions, PRK, LASIK, or IOL exchange for those surgeons in our practice who do not feel comfortable with these procedures.
The 2017 ASCRS clinical survey found that 84% of US surgeon respondents were very or extremely concerned about declining Medicare reimbursement.3 For this reason, the economics of presbyopia reimbursement play an important role in the future of healthy cataract practices. The fees for refractive cataract surgery that are set by individual practices are based on the work performed and the services provided by the practice.
No. 3: OFFER SOLUTIONS
In our practice, we have seen a steady growth in the adoption of presbyopia-correcting IOLs as the technology has improved with the addition of low-add multifocal and extended depth of focus lenses that improve quality of vision. We have also seen increased demand for laser cataract surgery.
The economic impact of refractive cataract surgery procedures is significant. In our practice, approximately 12% of patients receive a toric IOL and 10% receive a presbyopia-correcting IOL. Even though only about 22% of our patients receive a premium IOL, the revenue these procedures generate for our practice represents approximately 42% of the cataract surgery collections. More important, because refractive cataract surgery involves added labor but few associated added costs, this 22% of our patients who undergo refractive cataract surgery generates 61% of the cataract surgery profitability to our practice.
One of the important choices in offering refractive cataract surgery is whether or not to incorporate laser cataract surgery. To determine whether adding a femtosecond laser to cataract surgery is economically viable, we have to know the cost of buying and operating the femtosecond laser, including user fees and maintenance costs. The average price for a femtosecond laser device is $300,000 to $500,000, and the service fees on average are 10% per year. Additionally, systems have per-use fees that range from $350 to $450.
If we estimate on the high side of these ranges, the monthly cost of a laser cataract surgery system costing $500,000, paid over 60 months, will be approximately $10,000 per month. Variable costs include the procedure fee, staffing, and associated medications. The practice has to determine fees that can be economically viable for both the patient and the practice, and these fees must be documented to be reasonable compensation for the additional work and testing performed in association with the service provided.
Based on a $1,000 fee for laser cataract surgery, it would require approximately 25 patients per month to break even on this procedure. If it is projected that fewer than 25 procedures will be performed, the practice should consider adopting a roll-on/roll-off model rather than buying the equipment.
CONCLUSION
The most important concepts regarding the business of refractive cataract surgery are these: Always do what is best for the patient, give patients what they want, and perform surgery as safely as possible.
The key aspect that drives refractive cataract surgery is that it can offer better options for patients, including treatments that are customized to the patient to address individual demands and lifestyle. At the same time, we must have the ability to reduce side effects and perform enhancements when needed.
As our technologies have improved, patient demand for and adoption of refractive cataract surgery has increased. As our surgical experience improves, we will become more comfortable with these procedures. I believe that, as third-party reimbursement continues to decline, now is the time to embrace refractive cataract surgery.
Refractive cataract surgery allows us to provide high-quality patient care and to give patients improved quality of life. New technologies and techniques will continue to improve outcomes and patient satisfaction and to drive practice growth.
1. Slomski A. The end of old. Merrill Lynch Advisor: Outlook. 2014. https://benefitplans.baml.com/Publish/Content/application/pdf/GWMOL/ARV8U5VP.pdf. Accessed February 28, 2019.
2. Ferrer-Blasco T, Montés-Micó R, Peixoto-de-Matos SC, González-Méijome JM, Cerviño A. Prevalence of corneal astigmatism before cataract surgery. J Cataract Refract Surg. 2009;35:70-75.
3. ASCRS Clinical Survey 2017. www.supplements.eyeworld.org/h/i/377037466-ascrs-clinical-survey-2017. Accessed March 8, 2019.

