



Keratoconus can be a visually debilitating disease, especially when it reaches moderate to advanced stages in young adults. The Athens protocol—CXL combined with excimer laser partial PRK—can provide reliable rehabilitation in these patients, stabilizing vision and strengthening the biomechanical qualities of the thinned cornea.
AT A GLANCE
- The Athens protocol can provide reliable rehabilitation in patients with moderate to severe keratoconus, stabilizing vision and strengthening the biomechanical qualities of the thinned cornea.
- The latest iteration of the Athens protocol includes cyclorotation compensation for topography-guided partial PRK as a first step.
- This approach has been a stable, predictable tool for addressing severe visual morbidity associated with moderate to advanced keratoconus in young adults in Southern Europe.
In a large comparative case series, my colleagues and I have shown that same-session partial topography-guided PRK with CXL is more effective than sequential PRK after earlier CXL. The refractive effects of the combined, same-day treatment have been impressive: Most patients obtained a CDVA of 20/40.1,2
This Athens protocol3 has evolved over time to include sequential same-session excimer laser epithelial debridement (50 μm), partial topography-guided excimer laser stromal ablation, and high-fluence (6 mW/cm2) UV-A accelerated (15 minute) CXL.
The latest iteration of the Athens protocol now includes cyclorotation compensation for topography-guided partial PRK as the first step for these highly irregular corneas. Next, a 50-μm PTK is performed for epithelial removal, and then mitomycin C (MMC) 0.02% is applied for 30 seconds to complete the protocol (Figure 1).
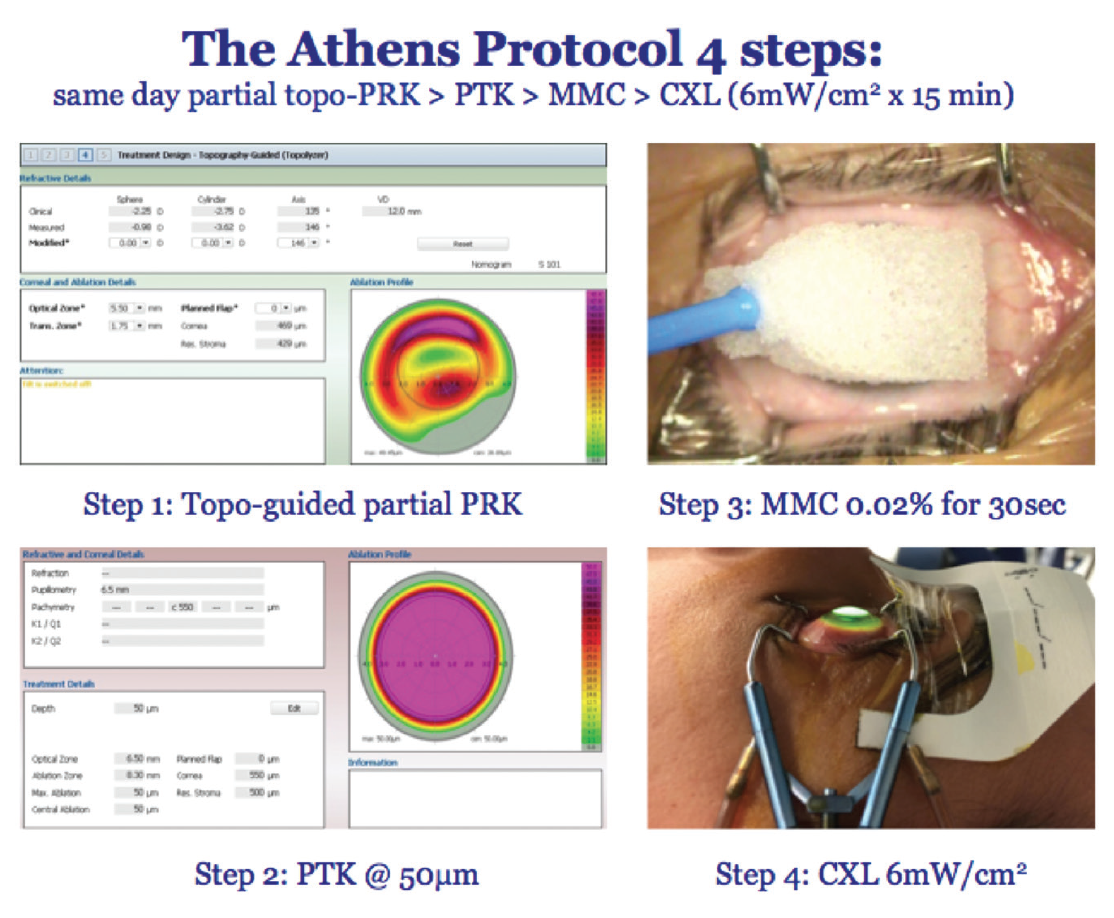
Figure 1. The four steps of the current Athens protocol.
DESIGNING THE ABLATION PATTERN
The most challenging part of the Athens protocol is designing the excimer laser ablation pattern. As this is not a refractive procedure, the priority is maximal normalization of the irregular anterior corneal surface caused by the thinned cornea.4 Therefore, the aim of the design is dual: (1) to reduce the large curvature of the cone area and (2) to attempt to relocate this steeper area to a more central location by steepening the flattened central cornea next to the cone.
In the planned ablation pattern in Figure 2A and the preoperative curvature data for the eye being treated in Figure 2B, the key distinct areas of this specific ablation pattern include the paracentral cone location (lower left), corresponding to the myopic ablation component.
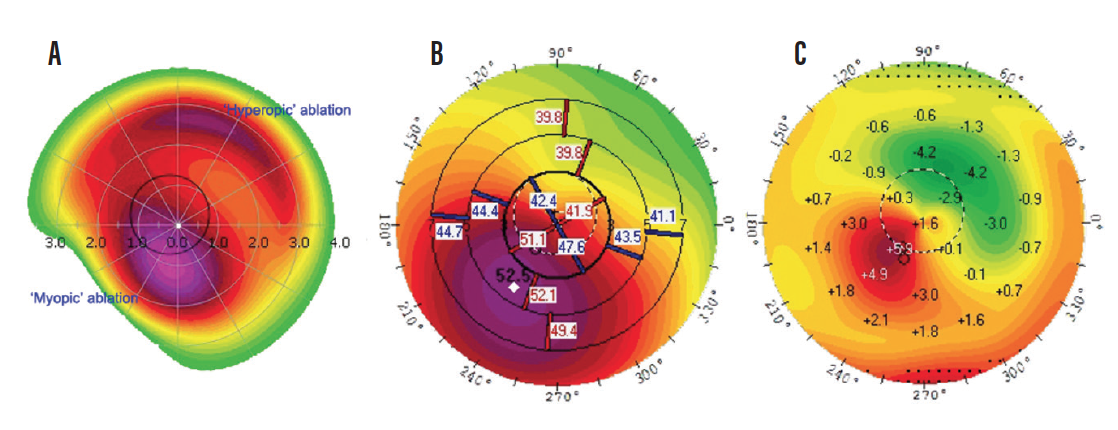
Figure 2. Topography-guided ablation pattern design (A); preoperative topography (B); difference between preoperative and 6-month postoperative topography (C). The angle in the difference map correlates with the intended ablation pattern, showing the myopic (red) and hyperopic (green) components of the achieved result.
The hyperopic ablation component (top right) corresponds to the antipode of the cone. The purpose of this second, hyperopic component is to create an artificial elevation gradient diagonal to the cone’s location.
Combining these two keratomileusis patterns, one hyperopic and one myopic, results in a dramatic reduction in corneal asymmetry, correlating clinically with a marked improvement in CDVA postoperatively.
CONCLUSION
Of course, this complex treatment may not be necessary in patients who can tolerate rigid gas permeable or scleral contact lenses. In our hands, however, it has proven to be the most stable, predictable tool for addressing severe visual morbidity associated with moderate to advanced keratoconus in young adults in Southern Europe.
We have reported and extensively published our early results,1 our late stability and visual rehabilitation results, and our results in pediatric patients, with only rare complications in 7- and 10-year follow-up.5 The fact that Athens protocol–type procedures have become the treatment of choice globally serves to further validate our findings.
1. Krueger RR, Kanellopoulos AJ. Stability of simultaneous topography-guided photorefractive keratectomy and riboflavin/UVA cross-linking for progressive keratoconus: case reports. J Refract Surg. 2010;26:S827-S832.
2. Stojanovic A, Zhang J, Chen X, et al. Topography-guided transepithelial surface ablation followed by corneal collagen cross-linking performed in a single combined procedure for the treatment of keratoconus and pellucid marginal degeneration. J Refract Surg. 2010; 26:145-152.
3. Kanellopoulos AJ. Long-term results of a prospective randomized bilateral eye comparison trial of higher fluence, shorter duration ultraviolet A radiation, and riboflavin collagen cross linking for progressive keratoconus. Clin Ophthalmol. 2012;6:97-101.
4. Kanellopoulos AJ, Asimellis G. Corneal refractive power and symmetry changes following normalization of ectasias treated with partial topography-guided PTK combined with higher-fluence CXL (The Athens Protocol). J Refract Surg. 2014;30(5):342-346.
5. Kanellopoulos AJ. Pediatric collagen crosslinking combined with partial topo-guided excimer normalization (Athens protocol) for keratoconus. Poster presented at: American Academy of Ophthalmology Annual Meeting; November 11, 2017; New Orleans.

