
We have both been offering the KAMRA corneal inlay (CorneaGen) at our practices now for about 2 years. Over the course of this time, we’ve homed in on the ideal preoperative refraction that allows the inlay to perform its best within the eye. That refraction is -0.75 D.
HOW IT WORKS
The KAMRA inlay is a laser-etched micro-disc with a hole in its center. The overall size is 3.8 mm in diameter, and the central opening is 1.6 mm. The design of the KAMRA inlay works much like a camera lens. The f-stop of a camera correlates to the size of the aperture, or the opening that controls the amount of light that penetrates the lens; the larger the f-stop, the smaller the aperture and, therefore, the more depth of focus it creates.
When a photographer takes a picture of objects at different depths, he or she would choose a high f-stop to increase the depth of focus and ensure that the objects in the front and those in the back all are in focus.
The KAMRA inlay works the same way, in that it incorporates a small aperture to increase depth of focus. Essentially that aperture eliminates blur by blocking peripheral defocused light, allowing more parallel rays of light to enter the eye. This system is ideal for enhancing near vision without sacrificing distance vision, which is exactly what our presbyopic patients are searching for.
WHY -0.75 D?
What has been found through studies and clinical investigations is that people who are -0.75 D preoperatively are the happiest KAMRA inlay patients. The reason for that is because the inlay extends the patient’s natural focus in both near and far directions (Figure 1).
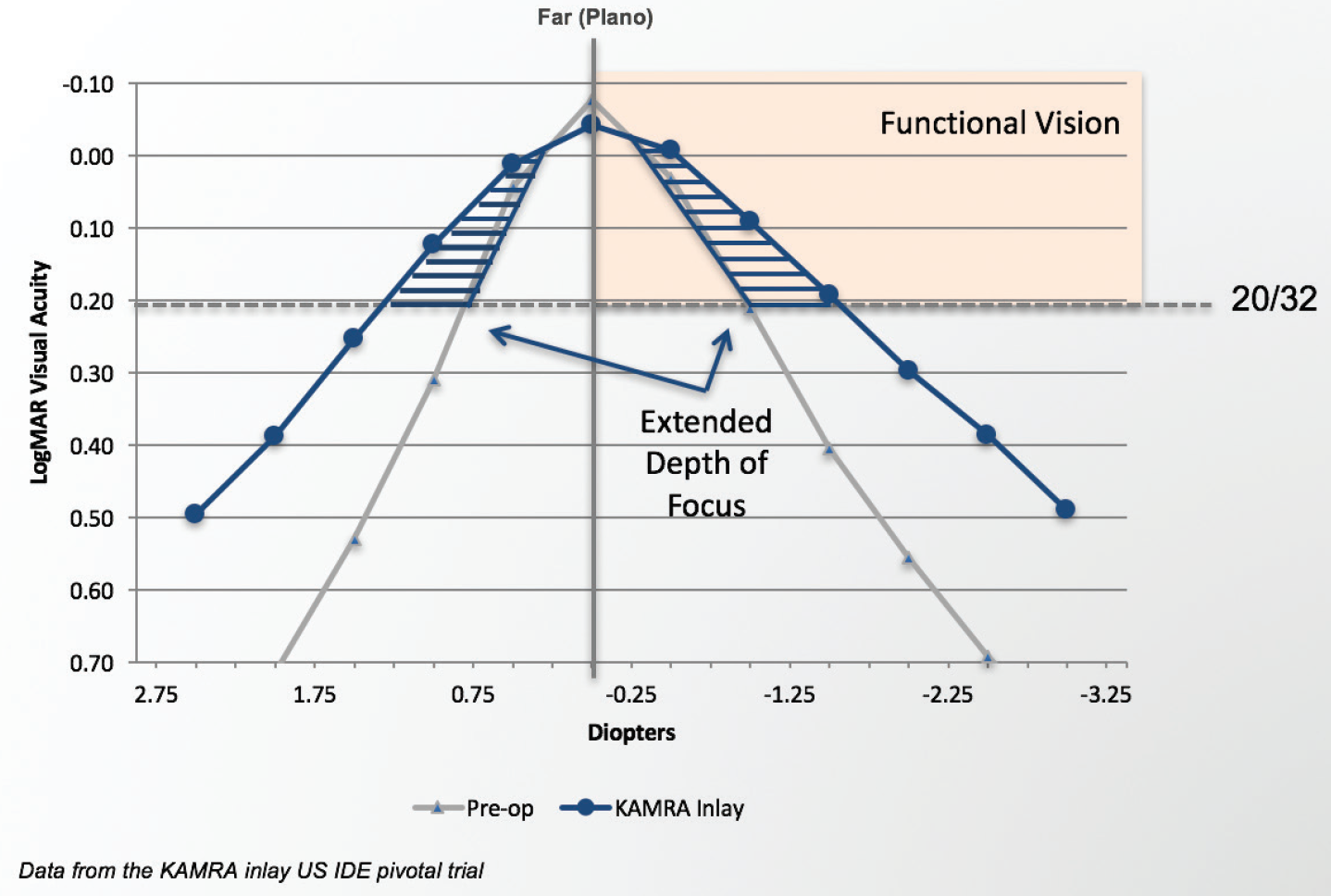
Figure 1. The small aperture flattens the existing defocus curve around the patient’s pre-existing MRSE, resulting in gains at near and far. When that MRSE is plano, the far vision benefit is not appreciated as it is added onto infinity. Near vision improves, but not necessarily to the degree desired by the patient.
In simpler terms, the KAMRA inlay promotes extended depth of focus and helps produce a visual acuity of about 20/25 at distance and J2 at near in the inlay eye. Having the KAMRA inlay extends patients’ focus back out on either side of their natural focus points and brings them in up close to boost near vision.
In plano patients, near vision will not be as strong as it is in -0.75 D patients (Figure 2). Likewise, in patients who are -0.50 D preoperatively, they will not fare as well as the -0.75 D patient, and they are more likely to be disappointed with their results. Furthermore, over time, the -0.50 D patient would start to lose some of his or her near vision. Therefore, whenever possible, we must get patients to -0.75 D before the KAMRA inlay is implanted. The result is that patients are able to maintain their near vision even longer (Figures 3 and 4).
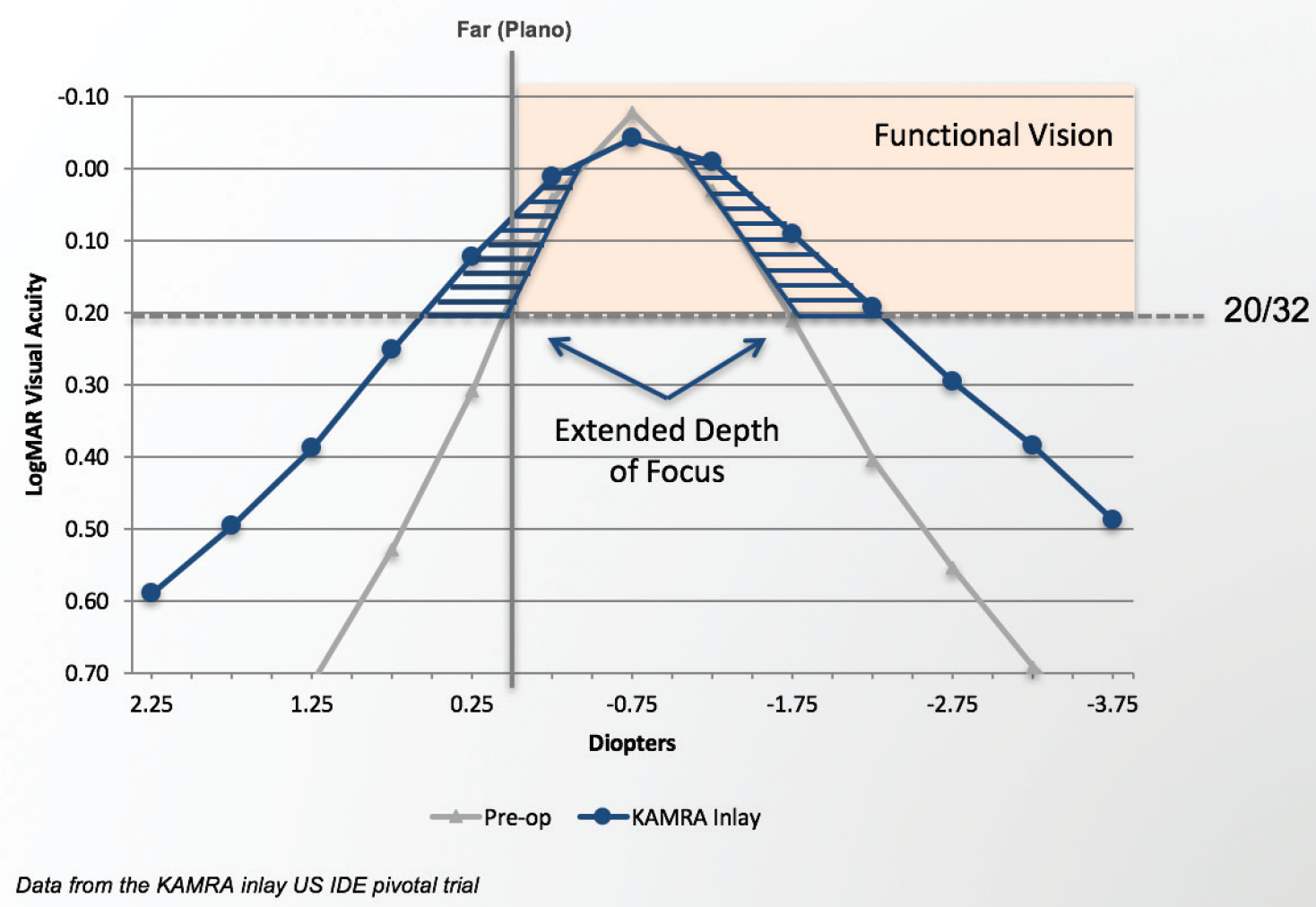
Figure 2. When the inlay eye has an MRSE of -0.75 D prior to implantation, more of the extended depth of focus provided by the small aperture is appreciated by the patient. Both far and near vision are improved.
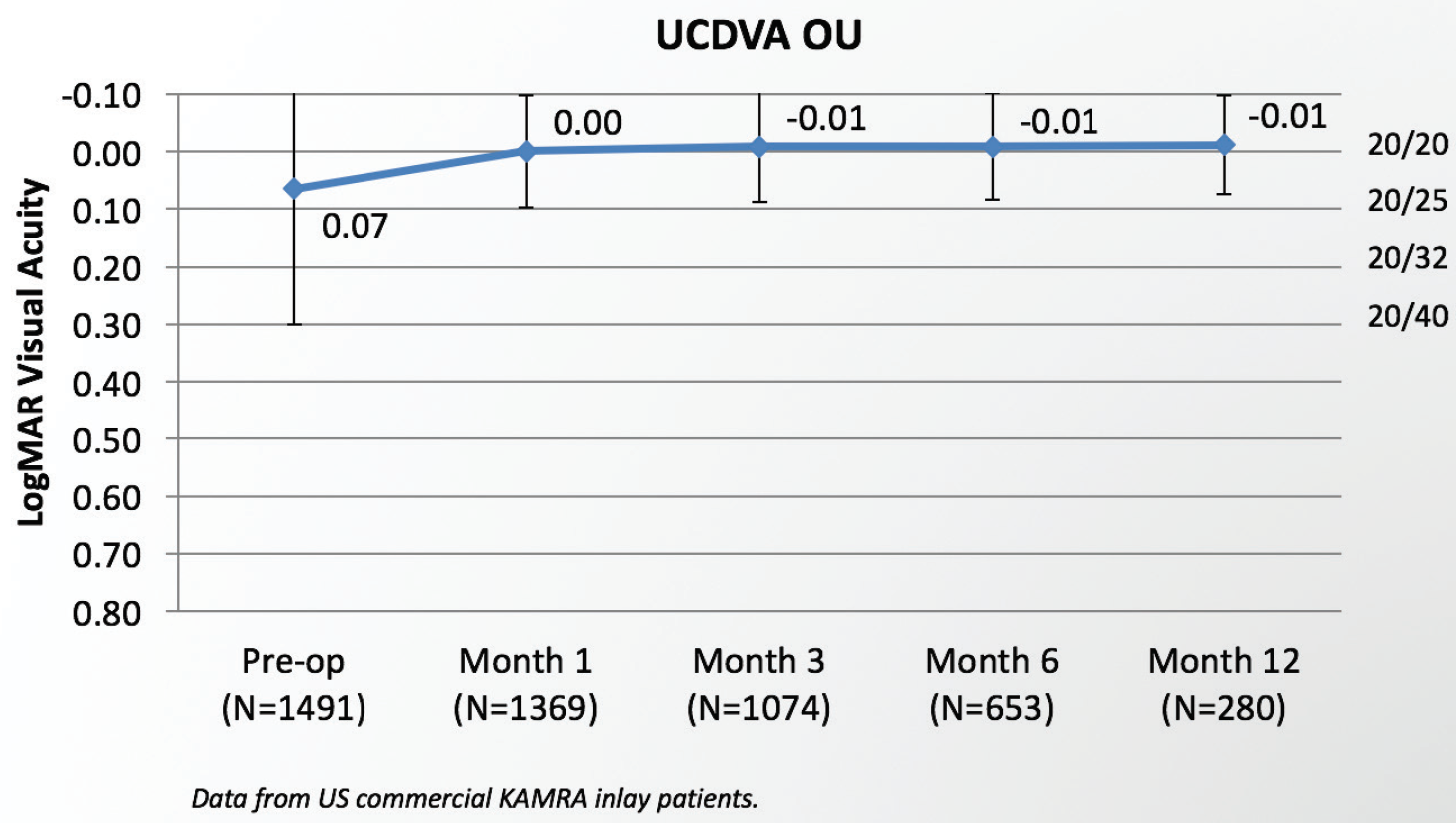
Figure 3. Patients maintain excellent distance vision over time after KAMRA inlay implantation.
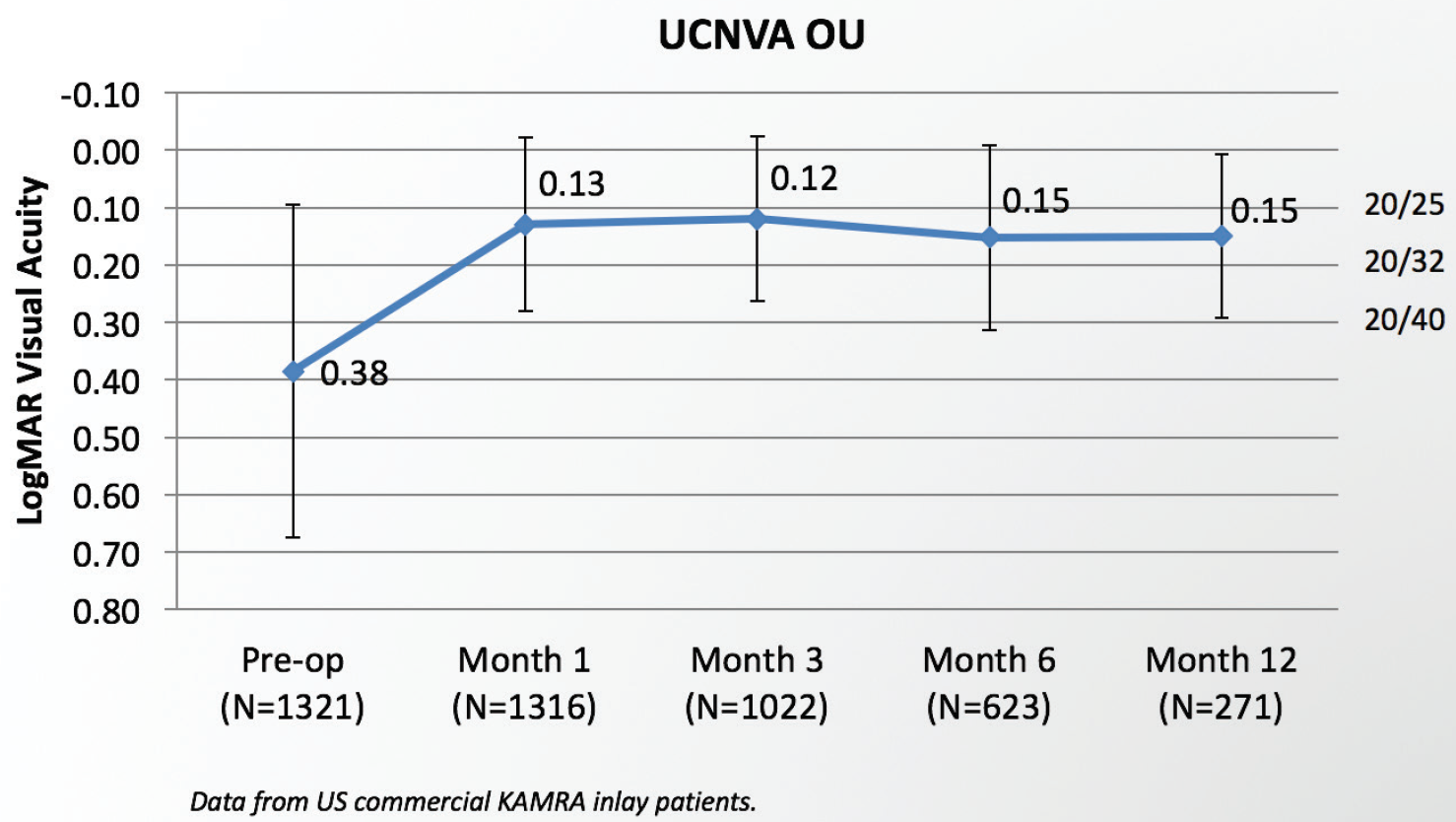
Figure 4. Patients achieve predictable, stable near vision after KAMRA inlay implantation.
CONCLUSION
The thing we like most about the KAMRA inlay is that it does not induce mini-monovision and, therefore, does not hurt distance vision. Rather, the KAMRA inlay can enhance near vision and slightly improve distance vision at the same time. I believe that the KAMRA inlay provides us with the best opportunity to get away from monovision and to give our patients near without sacrificing the distance.
KAMRA is a trademark of CorneaGen. All other trademarks are property of their respective owners.

