



Surgeons now have a range of IOL options for the correction of presbyopia. For years, we have had multifocal IOLs like the Tecnis Multifocal IOL, including the low-add models. Built on a single-piece IOL platform with the same high-quality, mid-index, low-dispersion material, the Tecnis Symfony and the Tecnis Symfony Toric Extended Range of Vision IOLs (Abbott) are the first and only extended-depth-of-focus (EDOF) IOLs approved by the FDA. With this diverse portfolio of presbyopia-correcting lens implants, surgeons can now choose an IOL that provides good far, intermediate, and near vision for patients with and without astigmatism.
To decide which one (or two) of these lens designs is right for a given patient, the surgeon must understand the strengths of the technologies and evaluate subjective and objective factors (see Subjective and Objective Factors to Consider for IOL Selection). If the patient is interested in spectacle independence, the first step is to identify which distances are most important to him or her for daily functioning.
Many cataract patients who work, drive, and are otherwise active have a preference for good intermediate vision over fine near vision. Similarly, tall patients and those with long arms tend to use their vision at intermediate more than near. Providing these patients great far and intermediate vision with good near vision allows them to function very well for most daily activities, including driving, using a computer, and looking at their tablet or smartphone.
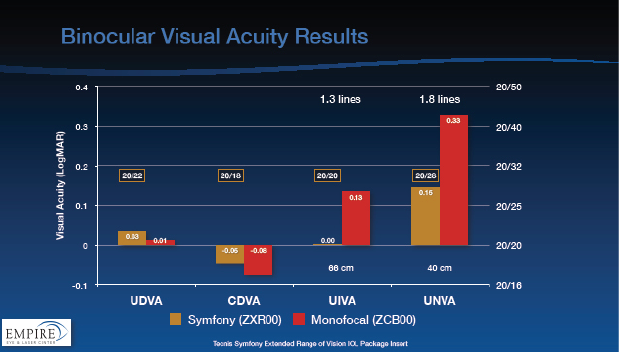
Figure 1. Patients with the Tecnis Symfony IOL can expect to achieve an uncorrected binocular visual acuity of around 20/20 for distance and intermediate and between 20/25 and 20/32 for near.
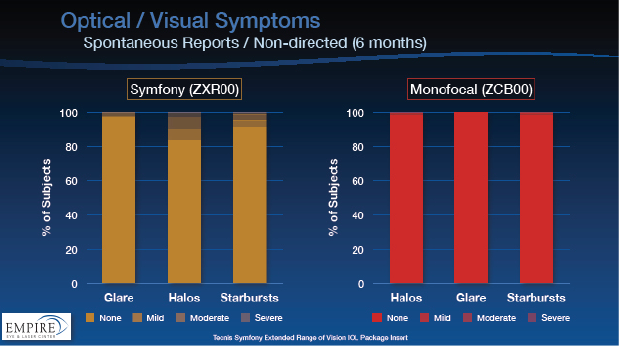
Figure 2. In the FDA study, less than 3% of Tecnis Symfony subjects noted severe night vision symptoms.
For these patients, the Tecnis Symfony IOL works very well. The only IOL that actively corrects chromatic aberration for far, intermediate, and near,1 the Symfony provides high-quality far vision as well as a continuous range of quality vision through intermediate and into near distance (Figure 1). The Symfony also minimizes night vision symptoms (Figure 2) and provides a certain amount of refractive forgiveness.
Older patients who do not drive much at night, those who read quite a lot, or individuals with specific fine-vision hobbies such as knitting or crafts may prefer a lens that puts more emphasis on near visual function. They may be willing to accept the potential tradeoffs in intermediate and night vision.
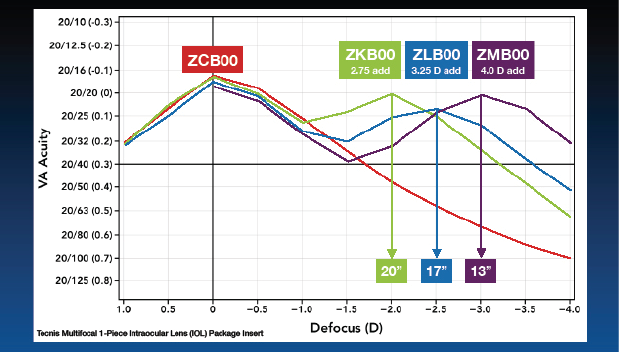
Figure 3. Clinical defocus curves of the Tecnis Multifocal Family of IOLs.
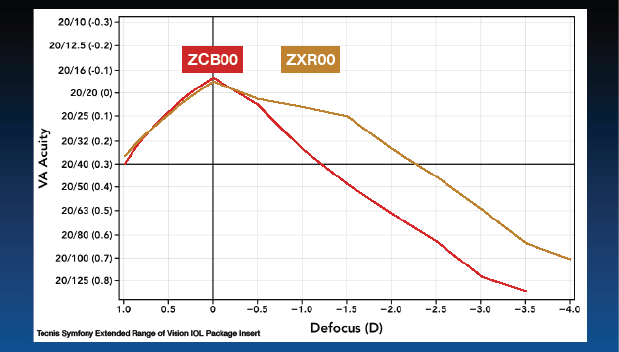
Figure 4. Binocular clinical defocus curves of the Tecnis Symfony IOL. A 1- to 2-line improvement in visual acuity over a monofocal lens was noted through ‑4.00 D of defocus.
Compared to an EDOF IOL, a multifocal IOL will provide better near vision. On the Tecnis Multifocal IOL platform, there is the traditional +4.00 D add as well as the newer low-add +3.25 and +2.75 D add versions, which I prefer for their improved night vision profile. The AcrySof Restor platform (Alcon) offers low-add versions as well; their poor chromatic aberration properties limits image quality, however, and their diffractive profile limits near visual acuity, particularly in dim light.2,3 Defocus curves for the monofocal, extended range of vision and all three multifocal add powers of the Tecnis lenses are shown in Figures 3 and 4.
FACTORS TO CONSIDER
First Eye
Fortunately, because they have so many options on one platform, surgeons are not required to choose the same IOL for both of a patient’s eyes. Unless one eye has a significantly worse cataract, I typically implant a Symfony lens in the dominant eye first. At the 1-day and 1-week postoperative visits, I assess the patient’s satisfaction with far, intermediate, near, and night vision to guide the IOL choice for the second eye.
Personality
The conventional wisdom is to be wary of engineers and others with exacting personalities. Although these patients can be difficult to please, their high-functioning reasoning allows them to understand and anticipate their result. I find that, the better I can educate them preoperatively, the better they will enjoy their outcome postoperatively.
Myopia
Surgeons should carefully educate patients with myopia. These individuals are typically accustomed to removing their glasses at near, so it is important to set proper expectations. Spending a little extra time preoperatively can be invaluable. In one recent case, I implanted a Symfony lens in the dominant eye of a -4.00 D myope. Because we discussed preoperatively the possibility of her desiring better near vision, it was not surprising that she wanted a +3.25 D Tecnis Multifocal IOL in the second eye. Postoperatively, she is very pleased with her far, intermediate, near, and night vision.
SUBJECTIVE AND OBJECTIVE FACTORS TO CONSIDER FOR IOL SELECTION
Subjective Factors
- Interest in spectacle independence
- Concern about night vision symptoms
- Occupation
- Hobbies
- Personality
- Expectations
- Satisfaction with first eye
Objective Factors
- Preoperative visual acuity
- Preoperative refraction
- Astigmatism—degree and regular versus irregular
- Ocular surface health
- Severity and type of cataracts (nuclear, cortical, or subcapsular)
- Comorbidities
- Height/arm length
Astigmatism
Patients with astigmatism used to present surgeons with a difficult choice between a toric lens with no presbyopic correction and a presbyopia-correcting lens with limited astigmatic correction. With the advent of the Tecnis Symfony Toric IOL, I can provide both. In fact, I rarely use a monofocal toric lens anymore. If a patient is going to have premium surgery, why not maximize his or her functionality with presbyopic correction?
CONCLUSION
It is great to have choices. It is even better when the new options provide broader flexibility and greater usability. Now, surgeons have a presbyopia-correcting IOL that has more refractive forgiveness than a monofocal IOL, providing another option to tailor presbyopic treatment to each patient.
1. Tecnis Symfony [package insert]. Abbott Park, IL: Abbott 2016.
2. Zhao H, Mainster M. The effect of chromatic dispersion on pseudophakic optical performance. Br J Ophthalmol. 2007; 91:1225-1229.
3. Acrysof IQ Restor Multifocal IOL [package insert]. Fort Worth, TX: Alcon 2016.

