In laser cataract surgery, the femtosecond laser is used to perform several functions, including creation of the capsulotomy, entry wounds, astigmatic incisions, and lens fragmentation. In the first three steps, surgeons primarily use the laser to improve the precision of what we can do manually. Lens fragmentation is unique in that it presoftens the lens, considerably altering the conditions that are present when we enter the eye with the phaco tip.
APPROACH VARIES BY DENSITY
Just as most surgeons have different phaco settings for soft and dense nuclei, I take different approaches in my laser pretreatment of the lens as well. In all cases, I use the laser to segment the lens, typically into quadrants. Each femtosecond laser platform has its own method for lens fragmentation. My system, the Catalys laser (Abbott Medical Optics), offers the surgeon choices in both the number of segments (quadrants, sextants, or octants) and the degree of softening to be performed.
The degree of softening with this laser can be controlled by decreasing the grid spacing or “cube” size. Grid spacing for the softening pattern can be adjusted from 100 to 2,000 µm. In very soft nuclei, segmentation alone is sufficient, and I do not perform any additional softening of the nuclear material. For a grade 1+ to 2+ nucleus, I use a 500-µm cubed grid, and for a grade 3+ to 4+ nucleus, I decrease the grid spacing to 300 µm for more intense softening.
In my practice, this approach has resulted in about a 70% reduction in ultrasound power compared to manual surgery across all grades of cataracts. Several studies have reported achieving significant reductions in effective phaco time (EPT), down to zero phaco power in many cases.1,2 In fact, some of the surgeons with the most experience with this technology have reported that, with some adjustments in their technique, settings, and instrumentation, they have been able to reduce EPT to zero in more than 90% of laser cataract surgery cases.3
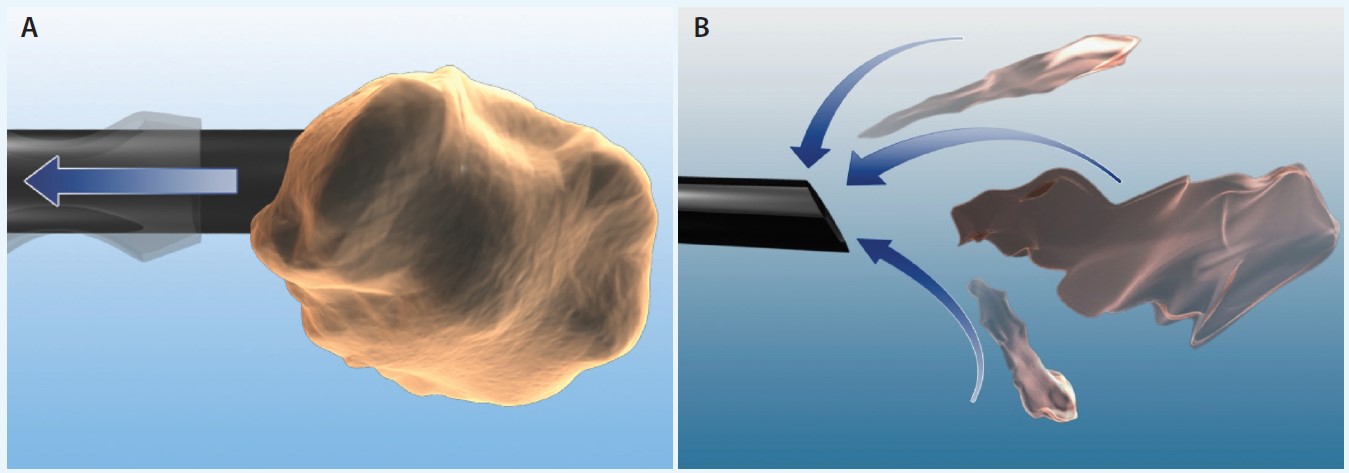
Figure 1. Occlusion in a peristaltic system creates strong holdability at the tip (A). When the lens has already been fragmented and softened, a high rate of flow is important (B).
This decrease in ultrasound energy should lead to a reduction in corneal edema, endothelial cell loss, and inflammation postoperatively, perhaps providing faster visual recovery. Although we have not yet tried to quantify these gains in our practice, my impression is that we have less trauma and clearer corneas in the early postoperative period in laser cataract cases compared to manual phacoemulsification.
Reducing surgical trauma is beneficial for all eyes, but there are certainly cases—including eyes with shallow anterior chambers, Marfan syndrome, pseudoexfoliation or zonular dehiscence, and corneal disease—where I already feel that laser surgery is the safest option for the patient. In someone with Fuchs dystrophy, for example, anything I can do to reduce phaco time and ultrasound energy makes me more confident that I can protect the cornea, keep the eye quiet, and return it to baseline more quickly after surgery surgery.
CHANGING FLUIDICS DEMANDS
In addition to the benefits to ocular tissues, the reduction in EPT means that I can perform a more fluidics-driven phaco procedure, with accompanying changes in surgical technique. I have different phaco systems available at the various surgery centers where I operate, so I can attest to the fact that laser cataract surgery can be performed with either a peristaltic- or Venturi-based phaco machine. However, my personal preference has swung to Venturi as the ideal companion for laser cataract.
Occlusion in a peristaltic system creates strong holdability at the tip, which is essential for holding on to large segments during chopping or divide-and-conquer maneuvers in a standard phaco procedure (Figure 1A). When the lens has already been fragmented and softened by the laser, holdability becomes much less important. Instead, I want a high rate of flow that will keep the smaller, softened nuclear fragments moving toward the tip. Venturi-style pumps excel at this (Figure 1B).
At a Glance
• The author takes different approaches in his laser pretreatment of the lens depending on the type of cataract. In all cases, he uses the laser to segment the lens, typically into quadrants.
• Presoftening the lens has resulted in about a 70% reduction in ultrasound power compared to manual surgery across all grades of cataracts in the author’s practice.
• Laser cataract surgery can be performed with either a peristaltic- or Venturi-based phaco machine. The author’s personal preference has swung to Venturi as the ideal companion for laser cataract surgery.
Using the WhiteStar Signature system (Abbott Medical Optics), I now typically begin a laser cataract surgery case in Venturi mode, which is very effective at drawing in nuclear fragments so I do not have to chase them around the chamber. I frequently switch pumps on the fly to use the peristaltic pump for cortical removal. Some surgeons find this stage of a laser procedure more difficult, because the cortex tends to be a little “stickier” than in a manual procedure. Here, the holdability of a peristaltic system can make it easier to grab cortex and strip it from the capsule. With the dual-pump capability, I do not find it any more difficult to remove cortex than in a standard procedure.
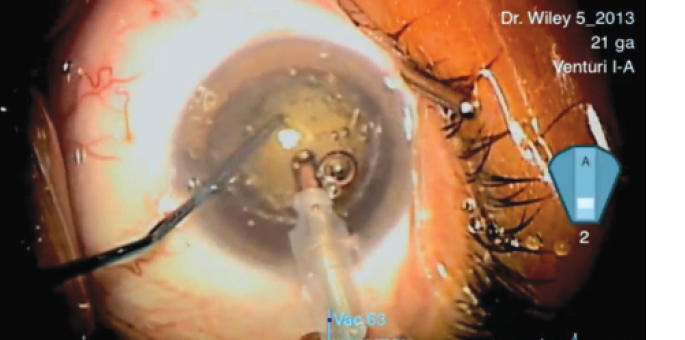
Figure 2. Zero-ultrasound extraction of a presoftened lens using the Catalys laser and dual-pump WhiteStar Signature phaco system (eyetube.net/v.asp?f=ogopi). Surgery performed by William Wiley, MD, with narration by Shamik Bafna, MD.
The accompanying video (Figure 2) illustrates the efficient aspiration of a moderately dense cataract in Venturi mode with no ultrasound energy, followed by cortical removal in peristaltic mode.
WHY LASER CATARACT?
A femtosecond laser is an expensive new device used to improve an already very good cataract surgery procedure. However, I believe this technology will provide the kind of incremental improvements we need to routinely get closer to LASIK results for our cataract patients. Laser surgery increases patients’ confidence in the surgeon and portrays the practice as cutting edge. Most importantly, the procedure is still in its infancy and likely to continue to distinguish itself further from manual surgery as the technology advances. n
- Conrad-Hengerer I, Hengerer FH, Schultz T, Dick HB. Effect of femtosecond laser fragmentation on effective phacoemulsification time in cataract surgery. J Refract Surg. 2012;28(12):879-883.
- Abell Robin G, Kerr NM, Vote BJ. Toward zero effective phacoemulsification time using femtosecond laser pretreatment. Ophthalmology. 2013;120(5):942-948.
- Dick HB, Schultz T. On the way to zero phaco. J Cataract Refract Surg. 2013;39(9):1442-1444.
Shamik Bafna, MD
• Cleveland Eye Clinic in Brecksville, Ohio
• (216) 287-2060; drbafna@clevelandeyeclinic.com
• financial disclosure: consultant to Abbott Medical Optics