

The Lensar Laser System with Streamline (Lensar) intelligently captures both pre- and intraoperative data to help optimize the safety and effectiveness of refractive cataract surgery. In my experience, the technology also improves workflow efficiency and reduces the risk of transcriptional errors.
Lensar with Streamline is the first laser cataract platform to allow the automation of several surgical planning and execution elements. Five new application upgrades include wireless integration with the Cassini Corneal Shape Analyzer (i-Optics), iris registration, cataract density imaging, customized fragmentation patterns, and arcuate incision planning. Imaging, planning, and guidance are organized, both before and during surgery, to optimize outcomes.
IRIS REGISTRATION
The acquisition of highly accurate preoperative corneal topography data and a high-definition infrared digital image of the iris' features help surgeons manage astigmatism effectively. The Cassini verifies the image's compatibility at the point of capture to minimize the risk of cyclorotation compensation failure once the patient is in the OR. Streamline then wirelessly transfers preoperative data from the Cassini to the laser, reducing the number of steps within the patient workflow and eliminating the need for staff to manually transfer the correct data via a memory stick. Automated data transmission to the Lensar patient-planning screen eliminates the potential for errors in transcription.
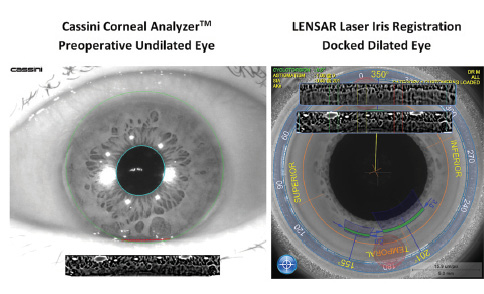
Figure 1. An 8.5° clockwise rotation was detected by iris registration and automatically compensated for during the incision-planning phase of the procedure.
Because cyclorotation is corrected after docking, the surgeon need not visually verify that the cyclorotation compensation is accurate, as required by some vessel-based tracking systems. Streamline's iris registration is not affected by the loss of vascular detail due to pharmacologic effects and automatically compensates for cyclorotation, improving refractive outcomes (Figure 1).1,2
PLANNING ARCUATE INCISIONS
The laser's arcuate incision-planning software autopopulates incision parameters based on the surgeon's preferences and surgically induced astigmatism (SIA). This feature can automatically recommend the placement of laser incisions based on preoperative data obtained with the Cassini. Alternatively, preoperative corneal topography data can be entered manually. In addition, the arcuate incision-planning software autopopulates incision parameters based on the surgeon's preferences and SIA; the steep axis corneal marking adds to the surgeon's ability to manage astigmatism.
This multiple data point planning tool is designed to optimize the construction of arcuate incisions by allowing modifications based on the patient's age and up to three additional parameters such as corneal white-to-white measurement, central corneal thickness, and corneal slope rate of change. Entries allow customization for toric IOL implantation. The Lensar is currently the only cataract laser system that provides this functionality directly on the laser, where real-time treatment planning decisions can be made.
At a Glance
• Recent upgrades to Streamline include wireless
integration with the Cassini, iris registration, cataract
density imaging, customized fragmentation patterns,
and arcuate incision planning.
• After docking, cyclorotation is corrected, and the
surgeon does not need to visually verify the accuracy
of the cyclorotation compensation.
• The arcuate incision-planning software autopopulates
incision parameters based on the surgeon's preferences
and surgically induced astigmatism; the steep
axis corneal marking further adds to the surgeon's
ability to manage astigmatism.
• The laser measures cataract density, defines
intralenticular morphologic boundaries, and applies
customized fragmentation patterns to minimize lens
extraction energy requirements.
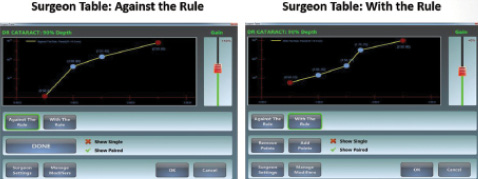
Figure 2. Against-the-rule and with-the-rule surgeon tables permit the entry of multiple data points for arcuate incision length and astigmatic power preference. The “gain” feature allows surgeons to adjust all data points by a specified percentage to account for under- or overcorrection.
Multiple planning metrics can be customized on an intuitive, user-friendly graphic interface. Metrics include incision depth with options for a fixed depth (250-900 µm), a fixed residual depth (0-900 µm), and percentage thickness (0%-100%). Against-the-rule and with-the-rule surgeon tables permit the entry of multiple data points for arcuate incision length and astigmatic power preferences (Figure 2). Moreover, surgeons can add several data points to better define arcuate incision planning such as single or paired arc treatments, modifiers, or their preferences. In addition, an age modifier gives the surgeon the option to adjust arcuate length using an age-based chart. Finally, with the incision placement pop-up box, the ophthalmologist can preoperatively adjust the locations for clear corneal incisions using surgeon tables and SIA information.
CATARACT DENSITY IMAGING
The Lensar laser's unique augmented reality imaging system identifies the boundaries between the endonucleus, epinucleus, and cortex in the lens. The surgeon can therefore automatically customize fragmentation patterns based on cataract morphology and density. Just as ophthalmologists manually performing phacoemulsification alter their parameters and techniques based on the structure and density of a cataract, the laser can now measure cataract density, define intralenticular morphologic boundaries, and apply customized fragmentation patterns to minimize lens extraction energy requirements.
Augmented-reality cataract density imaging (CDI) identifies the density and location of the nucleus within the cataract, much in the same way that Scheimpflug-based instruments perform lens analysis in the clinic.3 CDI enables preprogrammed surgeon-customized fragmentation patterns based on the density of the cataract, allows the surgeon to automatically isolate fragmentation to the nucleus, and facilitates proactive management of laser energy introduced into the eye.
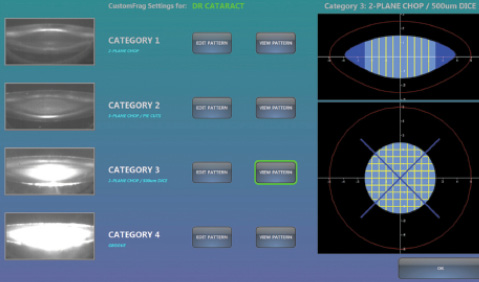
Figure 3. The surgeon programs patterns based on cataract morphology and surgical preferences. The laser maps each cataract and identifies density categories 1 through 4. CDI software auto-assigns predefined fragmentation patterns.
CDI eliminates the cookie-cutter approach of using the same fragmentation pattern for all densities of cataract without requiring laborious manual customization for each case (Figure 3). Multiple fragmentation parameter options are available, including one to four plane chops, sequential power level adjustments, and “pie” or “dice” patterns. In my experience, automated cataract density categorization and customized laser fragmentation improve operating efficiency and reduce energy requirements for lens extraction, promoting a smoother workflow and producing excellent outcomes for patients. n
1. Packer M, Klyce SD, Smith C. The Lensar Laser System–fs 3D for femtosecond cataract surgery. US Ophthalmic Review. 2014;7(2):89-94.
2. Chernyak DA. Iris-based cyclotorsional image alignment method for wavefront registration. IEEE Trans Biomed Eng. 2005;52(12):2032-2040.
3. Nixon DR. Preoperative cataract grading by Scheimpflug imaging and effect on operative fluidics and phacoemulsification energy. J Cataract Refract Surg. 2010;36(2):242-246.
Mark Packer, MD, CPI
• president, Mark Packer MD Consulting, Boulder, Colorado
• mark@markpackerconsulting.com
• financial disclosure: consultant to Lensar

