

Focal laser photocoagulation has been supplanted as the standard of care for patients with diabetic macular edema (DME); data showing the efficacy of antivascular endothelial growth factor (anti-VEGF) agents for this indication leave little room for argument. Laser treatment of microaneurysms can reduce visual loss compared with observation,1 but VEGF inhibition can actually yield significant gains in visual acuity.2 Ranibizumab (Lucentis; Genentech) has long been approved for the treatment of DME, and bevacizumab (Avastin; Genentech), frequently used off label for treatment of the disease, has been found to be equally effective when evaluated in smaller trials.3 Aflibercept (Eylea; Regeneron) is yet another effective option.4,5
However, there are patients who, for any number of reasons, cannot sustain the frequent treatment schedule required for anti-VEGF therapy. Once a patient misses a few visits, we basically have to start over in terms of managing his or her disease. With this segment of patients in mind, I was searching for an alternative therapy.
AT A GLANCE
• Other treatment options must be available for patients with DME who cannot sustain anti-VEGF therapy.
• Not every patient responds positively to micro- pulse laser therapy, but for those who do, it can be successful and minimize the treatment burden.
• A small study of patients with DME demonstrated a trend toward a more robust response to 532-nm micropulse laser therapy in pigmented eyes.
ENTER MICROPULSE LASER THERAPY
When I first learned about micropulse laser therapy for the treatment of DME, I was skeptical. I called it “The Emperor’s New Clothes,” after the story by Hans Christian Anderson, because the effect is not visible at the time of treatment—or often even 1 month following therapy. I soon found out that the emperor is not naked, as in the story; the treatment really does have an effect, even if the laser spots cannot be seen.
I was hesitant, but I was in need of an alternative therapy for select patients. A senior partner in my practice was in favor of adopting micropulse laser therapy, so we purchased the IQ 532 Laser System (Iridex). My first treatments produced lackluster results, prompting me to do additional research on power and duration settings so I could make adjustments. I started using two times the continuous-wave test burn, generally around 200 mW of power, and saw an improved response. My results at this low power setting made me more comfortable with the therapy, and I became more aggressive in my treatment parameters.
I began applying laser spots more confluently, directly over the fovea, and using higher powers. Once my first laser patients were 3 to 4 months out from initial therapy, I began to see significant improvements in their edema, and I gained the confidence to treat more of my patients with micropulse laser. Not surprisingly, not every patient responds positively to micropulse laser therapy, but for those who do, it can be tremendously successful and minimize their treatment burden.
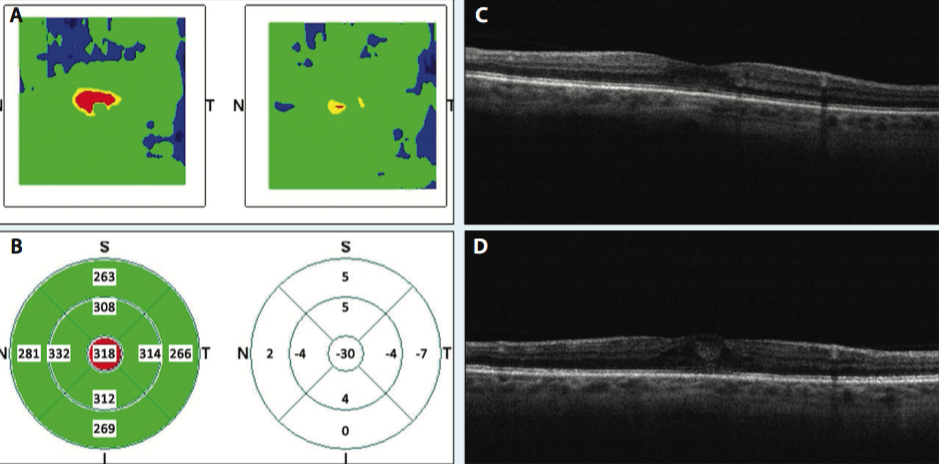
Figure. Optical coherence tomography (OCT) images of a 67-year-old woman with a 16-year history of well-controlled diabetes and mild blur in both eyes. Her left eye was 20/50 at presentation. She was unwilling to try injectable therapies, so primary micropulse laser treatment was applied. These OCT images represent her progress at 2 months after laser therapy. Color topography of central foveal edema improvement (A). Mathematical model calculation of central foveal thickness improvement (C). Spectral-domain OCT pretreatment foveal edema (C). Spectral-domain OCT posttreatment foveal edema improvement (D).
WHEN TO USE MICROPULSE LASER THERAPY
For those few patients with DME who have mild edema and 20/50 or better vision, I may try micropulse as primary treatment (Figure). For the majority of patients, however, I initiate DME therapy with injectable anti-VEGF agents. Once I observe a significant improvement and the patient’s central retinal thickness is less than 350 µm, I perform micropulse laser therapy. I then schedule a follow-up visit for 3 months so I can really see how effective laser therapy is. Patients love having a break from doctor visits as well.
For patients who do not respond sufficiently to injected anti-VEGF agents, I move to an implantable steroid such as the dexamethasone intravitreal implant 0.7 mg (Ozurdex, Allergan) or a 0.19-mg fluocinolone acetonide implant (Iluvien, Alimera Sciences). If the patient responds favorably to steroids, I may try micropulse laser therapy once I note a reduction in his or her central foveal thickness.
I have found that micropulse laser therapy may also be effective in some patients who do not respond to either anti-VEGF agents or steroids, and I will try this before resorting to vitrectomy.
TREATMENT PARAMETERS
I always begin laser treatment by first performing a continuous-wave burn outside of the area of edema. Starting at 80 mW of power, I titrate up until I see the gray-white effect of traditional focal laser. I then multiply the test burn power three times. (For example, if a patient responded to a 100-mW continuous-wave laser, I would perform micropulse at 300 mW with a 200-millisecond duration on a 5% duty cycle.) I do not use a duty cycle greater than 5% to minimize photothermic effects, especially with transfoveal treatment. For a 532-nm laser, I find that the power varies when performing the test burn, particularly because of pigmentation, so it is valuable to always perform a test burn first.
Also, because we do not have a dedicated slit lamp for our laser, we must set it up and remove it for treatment sessions. This constant handling can damage the fiberoptic cable, altering the applied power. Because there is no visible endpoint with micropulse laser therapy, I prefer to always perform my own initial safety check with a continuous-wave burn.
TECHNIQUE MODIFiCATIONS
My results improved once I made two adjustments to my technique. First, I treat directly over the fovea. This makes many surgeons nervous, but I have not had a single patient develop a scotoma secondary to treating over the fovea. Subjective and objective evaluation following treatment supports this claim.
The second change that improved patients’ outcomes was to increase the density of laser application. I now apply overlapping laser circles with a 5% duty cycle, and I have found that even confluent laser spots do not produce a burn that is visible clinically, angiographically, or tomographically. I recently tested the TxCell Scanning Laser Delivery System (Iridex), a new delivery system for micropulse laser treatment, and I found that patients have an easier time tolerating the treatment. It is also faster for the surgeon to apply treatment using this device.
A CLOSER LOOK
My partner and I conducted a small study of 62 patients who underwent 93 micropulse laser treatments using the IQ 532 laser.6 We both applied near-confluent density of 200-µm to 300-µm laser spots with the laser set to a 200-millisecond duration and a 5% duty cycle. My partner used a consistent 400 mW of power, while I titrated power to 2.5 times the continuous-wave test burn.
At follow-up between 3 and 6 months after treatment, we saw positive results. Overall mean visual acuity improved from 20/41 at baseline to 20/39 at follow-up, and central foveal thickness decreased from a mean of 343 μm at baseline to 325 μm at follow-up. While the significance of the visual acuity improvement is unclear, it must be noted that mean baseline visual acuity was excellent in this group of patients.
Closer analysis of our results provides some interesting insights. There was a trend toward a more robust response in pigmented eyes. In addition, patients with a posterior vitreous detachment and phakic eyes showed stronger results than their pseudophakic counterparts. We also learned that technique is important and that there is a learning curve when performing micropulse laser therapy. Reduction in central foveal thickness was significantly less in the first half of the study patients than in the second half. No eyes had angiographic evidence of photothermic burn following treatment, which is an important detail to note.
CONCLUSION
The diabetic population is increasing dramatically and with it the number of patients who must be treated for DME. Although anti-VEGF agents provide better results overall than any other single treatment, it is important to have a variety of options available so we can adapt therapy to the needs of each patient. Micropulse laser therapy has proven to be an important complement to anti-VEGF and steroid therapy for my patients with DME.
1. Early Treatment Diabetic Retinopathy Study research group. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Arch Ophthalmol. 1985;103(12):1796-1806.
2. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology. 2012;119(4):789-801.
3. Rajendram R, Fraser-Bell S, Kaines A, et al. A 2-year prospective randomized controlled trial of intravitreal bevacizumab or laser therapy (BOLT) in the management of diabetic macular edema: 24-month data: report 3. Arch Ophthalmol. 2012;130(8):972-979.
4. Korobelnik JF, Do DV, Schmidt-Erfurth U, et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology. 2014;121(11):2247-2254.
5. Diabetic Retinopathy Clinical Research Network; Wells JA, Glassman AR, Ayala AR, et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193-1203.
6. Luo C, Lin S, Neuwelt M. Micropulse: the Emperor’s new clothes. Paper presented at: The Asia-Pacific Academy of Ophthalmology Congress; April 1-4, 2015; Guangzhou, China.
Caesar K. Luo, MD
• board-certified vitreoretinal surgeon with Progressive Vision Institute in Pennsylvania (several locations)
• caesarluo@gmail.com
• financial interest: none acknowledged

