When the femtosecond laser was introduced for cataract surgery in 2010, it offered surgeons a novel way to access the capsule and fragment the cataract. For the skilled surgeon, however, this device initially was not a necessity.1 Today, that paradigm is shifting as advances in technology and techniques with the laser show definitive promise in giving the surgeon the ability to deliver authentically refractive outcomes beyond the power and positioning of the IOL.
In my opinion, the capabilities of one platform in particular help surgeons address and accommodate both potential surgically induced astigmatism and the inherent corneal cylinder prescription. The Lensar Laser System (Lensar) with its upgrades to Streamline is the first in the refractive cataract segment to address the specific challenges astigmatism presents in both the standard and premium lens channels. This article reviews the key features and benefits of the astigmatic treatment planning applications available to surgeons with this system.
AT A GLANCE
• Upgrades to Streamline allow surgeons to plan astigmatic treatments to be performed with the Lensar laser.
• Wireless data transfer, iris registration, and steep axis corneal landmarking improve surgeons’ efficiency and accuracy.
• The arcuate incision planning table allows surgeons to customize the location, depth, and extent of arcuate incisions based on the individual patient’s biometric measurements and the surgeon’s preferences.
WIRELESS DATA TRANSFER
A critical feature of the latest upgrades to the platform is the ability to transfer data wirelessly from popular topographers, including the Cassini (i-Optics) and the OPD III Scan (Marco Ophthalmics), to the Lensar laser. Not only does automated data transmission to the laser’s patient planning screen help to eliminate data transcription errors, it also reduces the number of steps within the patient flow and decreases the overall time of the procedure.
IRIS REGISTRATION
Another time-saving feature incorporated into the wireless data export from the Cassini is the qualification of the iris quality, which is conducted at the time of the preoperative examination (Figure 1).
The iris registration automatically compensates for cyclorotation by adjusting the placement of arcuate incisions. Cyclorotation errors as low as 4º can cause up to a 14% loss of astigmatic correction effect, and a 10º error can reduce the effect by 34%. Importantly, iris registration eliminates the need for surgeons to manually mark the eye, increasing the accuracy in placing incisions and avoiding the common problem of ink marks washing away.
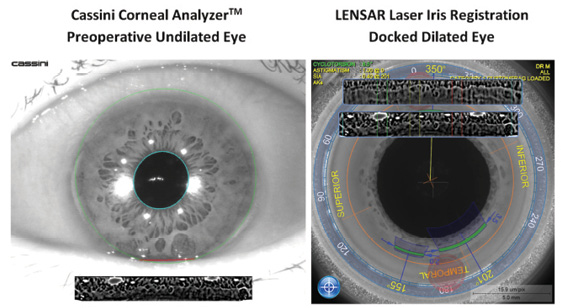
Figure 1. Advanced iris registration algorithms built into the Lensar platform map a patient’s iris from the undilated, preoperative image when the patient is sitting upright to the dilated surgical image taken once the patient is fully docked and in the supine position. The imagery is not affected by loss of vascular detail due to pharmacologic effects.
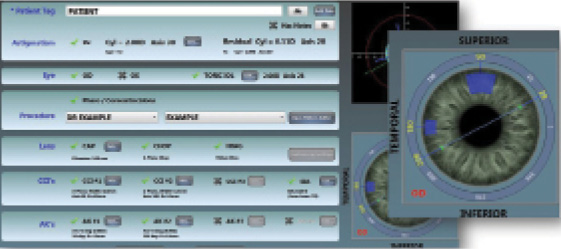
Figure 2. Lensar’s iris registration permits the construction of steep axis corneal marking to increase the surgeon’s flexibility in delivering astigmatism management modalities.
STEEP AXIS CORNEAL LANDMARKING
Another refinement to the platform is a steep axis corneal landmarking feature, Intelliaxis, which allows for the placement of nonrefractive corneal landmarks on the steep axis that are identified preoperatively from the corneal topographer or manual keratometer diagnostic scans (Figure 2). The Intelliaxis landmark incisions allow a surgeon to intraoperatively identify the steep axis under the surgical microscope after phacoemulsification, which is extremely valuable for toric IOL orientation.
REPRODUCIBLE RESULTS
When a surgeon makes the full commitment to performing arcuate incisions with the Lensar laser, it is critical that he or she perform the same astigmatic nomogram and streamlined approach for at least 50 eyes before changing his or her plan. Knowing one’s own surgically induced astigmatism (SIA) factor is another piece of the astigmatic puzzle needed to avoid under/overcorrections when treating astigmatism.
The calculator available on Dr. Warren Hill’s website (www.sia-calculator.com) is a very simple way for surgeons to assess their SIA prior to initiating astigmatic management planning with Streamline. Using data from the Cassini’s posterior corneal astigmatism measurements may also assist in a nomogram adjustment for total corneal astigmatic correction. Currently, Streamline only uses anterior corneal astigmatism data from the Cassini, but an adjustment can be made directly on the planning screen of the Lensar for posterior corneal astigmatism effect. Likewise, the Marco OPD III uses only anterior corneal astigmatism data for treatment planning purposes with the Lensar at this time.
ARCUATE INCISION PLANNING
The platform also includes an arcuate incision planning table for surgeons to customize the location, depth, and extent of arcuate incisions based on the individual patient’s biometric measurements and the surgeon’s preferences. The ability to save these planning tables within the platform affords greater efficiency in the OR. These two components—patients’ measurements and surgeons’ preferences—combine to effectively bring a new level of ease and precision to customizing corneal astigmatic treatment planning.
MY EXPERIENCE
In a noncomparative case series evaluating the treatment of corneal astigmatism using arcuate incisions created with the Lensar during cataract surgery, I treated 52 eyes of 31 patients with preexisting astigmatism ranging between -0.40 and -2.75 D. There was a significant reduction in mean absolute values of refractive astigmatism from 1.30 to 0.30 D (P < .001). Correspondingly, vector analysis of refractive cylinder also revealed an improvement in the J0 and J45 vectors. There were no complications, suggesting that the laser is a safe and effective treatment option for correcting astigmatism with arcuate incisions.
FINAL THOUGHTS
What impresses me most about Lensar’s approach to laser cataract surgery is the drive toward innovation that supports surgeons’ and patients’ satisfaction with the procedure. Improved efficiencies, greater customization, and specific attention directed toward the ability to effect refractive improvement beyond the power of a well-placed lens are all attributes that will solidify the appeal, adoption, and conversion to refractive cataract procedures with a laser. With markerless iris registration and topographer-enabled total corneal astigmatic analysis, Streamline brings the customization of astigmatic correction on the cornea to the next level of precision and efficacy in my opinion.
1. Donaldson KE, Braga-Mele R, Cabot F, et al. Femtosecond-laser assisted cataract surgery. J Cataract Refract Surg. 2013;39(11):1753-1763.
Mitchell A. Jackson, MD
• founder and CEO, Jacksoneye, Lake Villa, Illinois
• mjlaserdoc@msn.com; Twitter @djmjspin
• financial disclosure: consultant to i-Optics, Lensar, Marco Ophthalmics