
CASE PRESENTATION
A 13-year-old boy is referred for cataract surgery 1 month after a traumatic injury to his left eye from a paintball. The patient wore eye protection equipment, but he pulled down his goggles reflexively after they were obscured by paint, whereupon he was hit in the eye by another paintball. His UCVA has worsened steadily after the injury and is 20/200 OS on presentation. He reports mild discomfort in his left eye. Examination findings for the emmetropic right eye are entirely within normal limits.
A reverse pupil evaluation on a swinging flashlight test of the left eye is performed with log unit neutral density filters to account for the patient’s iridoplegia and fixed 7-mm pupil. No relative afferent pupillary defect is detected. Three clock hours of superotemporal iridodialysis are observed. The left eye projects light accurately. The IOP is 15 mm Hg OS on a regimen of two topical glaucoma drops and one topical steroid administered four times per day. The anterior chamber is formed. Gonioscopy finds an open angle with pigment. The crystalline lens is rapidly becoming intumescent, partially obstructing the view of the fundus. B-scan ultrasonography shows a hint of lens material behind the posterior capsule and no retinal detachment. A knuckle of vitreous may be protruding through the superotemporal zonulolysis and into the anterior chamber.
How would you proceed?
— Case prepared by Lisa Brothers Arbisser, MD

KENDALL E. DONALDSON, MD, MS
Anterior segment OCT imaging and high-resolution B-scan ultrasonography would be performed to evaluate the lens for tilt consistent with severe zonular instability and look for lens material posterior to the capsule. In preparation for surgery, all possibly appropriate tools would be made ready, including trypan blue dye, a capsular tension ring (CTR), a vitrectomy setup, sutures for repairing the iridodialysis, and needles for fixation of the IOL with the Yamane technique.1 Various lens options would be on hand, including a one-piece IOL for placement in the bag, a three-piece IOL powered for sulcus positioning, and a CT Lucia (Carl Zeiss Meditec) for potential fixation with the Yamane technique.
The case would be scheduled toward the end of an OR day to allow ample time and reduce stress. I would consider using a femtosecond laser to create the capsulotomy because doing so should minimize stress on the zonules from capsule manipulation. Another advantage of a femtosecond laser is OCT imaging, which would facilitate an evaluation of the posterior capsule's integrity. The laser system would also permit centration of the capsulotomy to be offset if the capsular bag complex has been displaced.
Capsular staining with trypan blue dye could be useful if the cataract is white and soft and it obscures visualization of the red reflex. It is important, however, not to instill an abundance of the dye because it may sneak around compromised zonules to stain the vitreous and obscure the red reflex.
A copious amount of a dispersive OVD would be instilled to help prevent vitreous prolapse. A limited conjunctival peritomy would then be performed in the area of the iridodialysis. A double-armed 10-0 polypropylene suture (Prolene, Ethicon) on a straight STC-6 needle would be passed from either a paracentesis or the temporal wound (depending on the distance from the primary wound to the iridodialysis) to an exit wound located approximately 2 mm posterior to the limbus in the central area of the iridodialysis to reposit the iris. My preference is to thread the suture into the bevel of a 27-gauge needle passed into the anterior chamber because it can be difficult to judge the exit position of a blind pass. Repairing a large iridodialysis before cataract removal creates more space for phacoemulsification. Repair would be paused several times for the reinstillation of a dispersive OVD to prevent vitreous prolapse.
If vitreous is presenting, I would consider removing the cataract with a vitrector. In situations like this one, the lens is soft and typically can be aspirated. As lens material is removed, the view to the posterior capsule should become clear, and any defect can be evaluated. The vitreous face is usually stable in a child, but a posterior capsulotomy can be considered if a small defect is present. Placement of the IOL in the capsular bag would be attempted. If zonular instability in the region of the iridodialysis is evident, then a CTR would be inserted.
If a significant amount of vitreous is present in the anterior chamber and the bag cannot be salvaged, then a limited pars plana vitrectomy would be performed. (Infusion would be performed through a paracentesis in the anterior chamber, and a vitrector would be placed 2.25 mm posterior to the limbus.) A CT Lucia (with IOL calculations performed for placement in the bag) would then be fixated using the Yamane technique. Two ultrathin 30-gauge TSK needles would be inserted 3 mm posterior to the limbus and tunneled parallel to the limbus for 2 mm before entering the anterior chamber. Low-temperature cautery would be applied to secure the haptics (without touching them) 180º apart.
Fortunately, the patient is past the age of amblyopia, and the axial length of the eye has likely reached nearly its full extent. These factors simplify the postoperative course and avoid issues related to anisometropia because the other eye is emmetropic.

SOOSAN JACOB, MS, FRCS, DNB
After an intraoperative assessment of the eye, an iris hook would be placed to hold back the iris. A trocar anterior chamber maintainer would then be placed, and an intravitreal triamcinolone acetonide–assisted vitrectomy would be performed to address prolapsed vitreous in the anterior chamber. The exact status and size of the posterior capsular tear are unknown, so a lensectomy with a glued IOL would be my backup procedure. First, however, I would tentatively explore the possibility of creating a capsulorhexis sized and centered for potential optic capture.
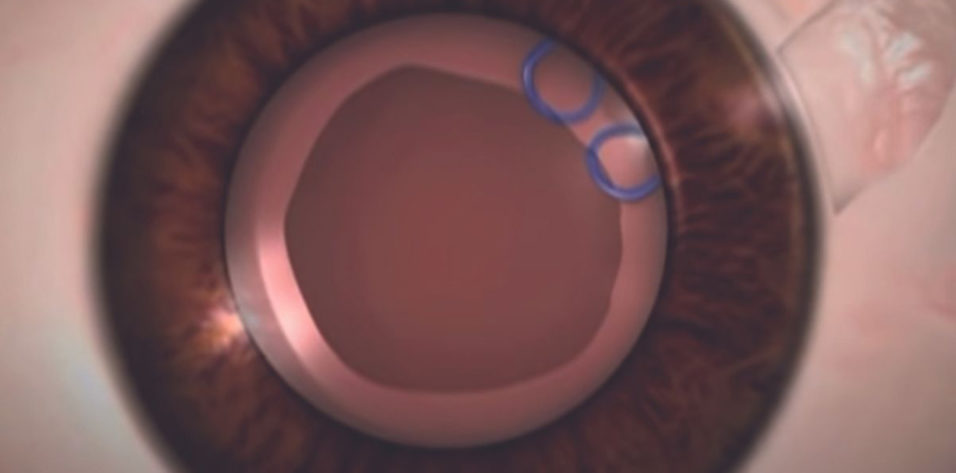
Soft lens matter would be removed with either a Simcoe cannula or an I/A probe set at a low flow rate. A CTR and a glued capsular hook2 or paper-clip capsule stabilizer (Figure) together with conventional capsular hooks would be placed depending on the extent of zonular dialysis (see videos below to view demonstrations of two of these techniques).
Figure. The paper-clip capsule stabilizer engages the capsular rim. The haptic is externalized via a sclerotomy and then tucked into an intrascleral Scharioth tunnel.
A glued capsular hook would provide intra- and postoperative support to the bag. Conventional hooks would enhance intraoperative support. If the tear in the posterior chamber is small, then it would be converted into a posterior capsulorhexis, and the IOL would be implanted in the bag. If the tear is large and the capsulorhexis is centered, then optic capture would be performed. If the capsulorhexis is decentered, then a supracapsular glued IOL3 would be placed just anterior to the capsular bag. If none of these procedures proves feasible, then I would consider performing a lensectomy and a glued IOL.4
The iridodialysis would be repaired with a double-armed 10-0 polypropylene suture. The size of the pupil would be reduced with either four-throw pupilloplasties5 or iris cerclage.

CATHLEEN M. MCCABE, MD
The vitreous in the anterior chamber would be addressed first to lessen the risk of an iatrogenic retinal break. I prefer to sit temporally, so superior and inferior paracentesis incisions would be created. The anterior chamber would be filled with a dispersive OVD, an additional paracentesis would be created nasally at an angle, and an anterior chamber maintainer would be placed. Two additional paracentesis incisions would be made in the area of the iridodialysis to permit the placement of iris hooks. Next, an anterior vitrectomy would be performed from an anterior approach to remove prolapsed vitreous. The anterior chamber would be refilled with a dispersive OVD. I generally prefer to place 23-gauge trocars at the start of the surgery and perform the vitrectomy from a pars plana approach. The view here, however, is compromised by a dense cataract. I would start from an anterior approach.
An OVD would be instilled to tamponade the area of zonulopathy, prevent further vitreous prolapse, and push away the iris. Iris hooks would be placed to keep the iris away from the phaco handpiece. A continuous curvilinear capsulorhexis (CCC) would be initiated by piercing the capsule centrally with a 27-gauge needle—its bevel down—and a small amount of liquified cortex would be aspirated to decompress the capsular bag. The CCC would then be completed with fine Utrata forceps. If necessary, intraocular forceps would be used to provide countertraction in the area of the zonulopathy. Alternatively, a femtosecond laser or the Zepto Capsulotomy System (Centricity Vision) could be used for the capsulotomy.
When a ruptured capsule is suspected, I find it best to avoid hydrodissection and perform little to no hydrodelineation. Low flow settings would be used to prevent an extension of a posterior capsular tear. The central nucleus—likely soft in a patient this age—would be debulked, and viscodissection of the epinucleus and cortex would be performed to prevent additional vitreous prolapse. It may be possible to completely remove the nuclear material and cortex with bimanual irrigation and aspiration alone.
The posterior capsule would be inspected to determine if an IOL can be safely placed in the capsular bag or if sulcus placement with optic capture is preferable. A CTR can be inserted atraumatically with a Sinskey hook placed through the leading eyelet if the posterior capsule is intact or the tear is stable and fibrosed. If the capsule is intact, then an aspheric CT Lucia IOL would be implanted. If zonular stability is questionable or a posterior capsular tear is detected, then I would proceed in one of two ways. Either a three-piece IOL would be placed in the sulcus and the optic captured or the Yamane technique for intrascleral haptic fixation would be used.
A conjunctival peritomy would be created superotemporally in the area of the dialysis. A crescent blade would be used to make a partial-thickness groove incision parallel and 1.5 mm posterior to the limbus. A double-armed 10-0 polypropylene suture would be passed through a paracentesis and used to engage the iris root and reapproximate the iris to the sclera. The needles would be externalized through the previously created groove, and the knot would be rotated to bury it fully in the scleral groove. Alternatively, a 6-0 or 7-0 polypropylene suture preloaded into a long 27- or 30-gauge needle could be passed through a paracentesis and used to loosely reapproximate the iris root to the sclera with a sewing machine technique. Flanges would be created with low-temperature handheld cautery.6 It would be important to avoid tight reapproximation of the iris to the sclera. Instead, a small space between the two tissues would be maintained. Carbachol intraocular solution (Miostat, Alcon) would be instilled in the anterior chamber to demonstrate the degree of mydriasis, which could be managed with interrupted sutures using a four-throw pupilloplasty technique.7 Alternatively, a pupillary cerclage could be performed.
Finally, a goniotomy would be performed nasally. Diluted triamcinolone acetonide would be injected into the anterior chamber to identify any vitreous. An additional vitrectomy would be performed if necessary. Intracameral moxifloxacin would be administered. The peritomy, if created, would be closed with bipolar cautery or an 8-0 polyglactin suture (Vicryl, Ethicon). A drop of a topical IOP-lowering medication would be instilled. The patient would be cautioned not to rub the eye. Follow-up examinations would include IOP monitoring, OCT imaging to assess the thickness of the retinal nerve fiber layer (although normative data for a 13-year-old are not available), and a visual field test if abnormalities are present.

DANIEL TERVEEN, MD
Surgery would be performed under monitored anesthesia care with a retrobulbar block. A peritomy would be made in the area of the iridodialysis. The eye would be marked for both a sutured Ahmed Segment (FCI Ophthalmics) and horizontal mattress sutures for iris repair. Triamcinolone acetonide would be instilled in the anterior chamber to indicate the amount of vitreous present. A combination of dispersive and cohesive OVDs would be instilled in the area of vitreous prolapse and dialysis to push back and tamponade the vitreous.
The iridodialysis would be repaired with 9-0 polypropylene sutures passed in a horizontal mattress fashion to keep back the iris during lens removal. The anterior capsule would be painted with trypan blue dye and evacuated with additional amounts of a dispersive OVD injected as needed to keep the anterior chamber pressurized. A 5-mm anterior capsulorhexis would be performed. The lens would then be viscodissected and removed with low-flow irrigation and aspiration.
At this point, the integrity of the posterior capsule would be evaluated to determine if the lens material observed is from a rupture or oncotic pressure due to the tumescent cataract. If a posterior capsular defect is present, then the capsular bag would be inflated with an OVD. An attempt would be made to create a posterior capsulotomy of equivalent size to the anterior capsulotomy. A CTR would be placed in the equator of the capsule, and an Ahmed Segment would be secured in the area of the zonular dialysis with a PTFE suture (Gore-Tex, W.L. Gore & Associates; off-label use).
A one-piece acrylic IOL would be implanted if the capsule is intact. Otherwise, a three-piece IOL would be placed in the sulcus, double optic capture would be performed, and the haptics would be positioned 90º from the eyelet of the Ahmed Segment.
Most of the OVD would be removed, but a small amount of a dispersive OVD would be left in the area of the repaired dialysis. Standard intracameral injections of antibiotics and steroids would be performed.
Because the injury occurred only 1 month ago, management of the fixed, dilated pupil would be delayed for 3 to 6 months. Several thorough retinal examinations would be performed during that time. If the retina is stable and the patient is cleared by the retina service, then an iris cerclage would be performed. If the IOP is elevated, then trabecular microbypass stents would be placed.
The biggest variables in the case are the stability and integrity of the capsule and the behavior of the vitreous. If the vitreous cannot be managed with tamponade, then I would have a low threshold for placing a trocar and amputating the prolapsing vitreous with a vitrector.


ABHAY R. VASAVADA, MS, FRCS(ENGLAND), AND DEEPA AGRAWAL, MS
First, we would have a long discussion with the patient’s family about the nature and extent of his injury. We would explain that the technical and functional outcomes of surgery are limited after such a severe injury, and we would emphasize the patient’s need for lifelong monitoring for glaucoma and retinal complications. It is important to ensure that the family has realistic expectations regarding surgery.
Ultrasound biomicroscopy might help to identify vitreous herniation, zonular dialysis, and perhaps even a posterior capsular rupture.
Surgery would be performed under general anesthesia. A vitrectomy is necessary, so a trocar would be introduced 4 mm behind the limbus in the inferotemporal quadrant at the beginning of the surgery. Iridodialysis and zonular dialysis is evident in the superotemporal quadrant, so a 2 x 2-mm partial-thickness scleral flap would be made for the repair. Preservative-free triamcinolone acetonide would be injected through a 1-mm paracentesis to identify vitreous in the anterior chamber. The anterior capsule would be stained with trypan blue dye. A dispersive OVD with a high molecular weight (Viscoat, Alcon) and a cohesive OVD (either Healon GV or Healon5, both from Johnson & Johnson Vision) would be used to tamponade the vitreous prolapse. A CCC would be performed, and lens material would be removed with closed-chamber bimanual irrigation and aspiration under direct visualization. A pars plana vitrectomy would then be performed.
Further management of the posterior capsule and IOL fixation depend on the integrity of the posterior capsule and capsular bag complex. A small tear in the posterior capsule would be converted into a continuous posterior capsulorhexis, and a three-piece IOL would be implanted in the bag. If a large tear is found in the posterior capsule, then a three-piece IOL would be implanted in the sulcus, and the optic would be captured through the anterior capsulorhexis. If only zonular dehiscence is found, then the bag would be secured with a Cionni CTR (FCI Ophthalmics) fixated under the scleral flap with a PTFE suture. A one- or three-piece IOL could then be implanted in the bag. If the posterior capsule is torn and zonular dehiscence is evident, then the bag would be removed, a vitrectomy would be performed, and scleral fixation of the IOL would be performed with the Yamane technique.
Next, a limbal paracentesis would be made opposite the iridodialysis. A double-armed 9-0 polypropylene suture would be fed through the paracentesis, passed through the iris root and the anterior chamber angle, and tied on the surface of the globe under a partial-thickness scleral flap. Alternatively, using a railroad technique, a 27-gauge needle could be passed through the scleral bed and used to externalize the 9-0 suture.
In advance of efforts to create a cosmetically acceptable pupil, a retina colleague would be asked to assess the peripheral retina with a retinal viewing system. (In our practice, pupilloplasty is considered for eyes with more than 5 to 6 mm of mydriasis.) A pupilloplasty would be performed using a modified four-throw Siepser knot at two positions 180º apart. The goal would be to achieve a pupil size of 2 to 3 mm.
The main incision would be closed with interrupted 10-0 nylon sutures. Triamcinolone acetonide would be injected into the anterior chamber to identify residual vitreous. The OVD would be removed, and an intracameral injection of preservative-free moxifloxacin would be performed.

WHAT I DID: LISA BROTHERS ARBISSER, MD
The case occurred during the days of 20-gauge vitrectomy—before the FDA approved trypan blue dye and before surgeons routinely stained the vitreous for particulate identification.
After extended counseling, the patient and his family decided to proceed with cataract surgery. The target was emmetropia. It was planned that he would wear safety glasses with progressive lenses postoperatively. I prepared him and his family, however, for the possibility of aphakia.
General anesthesia was administered because of the patient’s age, the need to sew the iris, and the uncertainties of the case. A dry technique under OVD control was used because there was a distinct possibility that the posterior capsule was open. After the creation of a carefully sized CCC, the flocculent lens material was aspirated with a 26-gauge cannula on a 3-mL syringe through a paracentesis (with a closed main clear corneal incision) under a soft shell of dispersive and cohesive OVDs. A small bounce of the anterior chamber was observed as the first bit of central lens material was aspirated, indicating the presence of a traumatic opening in the posterior capsule. (See video below to watch the case.)
The cannula was exchanged for a vitrector placed through the paracentesis for aspiration, and the eye was refilled with an OVD as necessary to maintain normotension. The vitrector was angled downward through the posterior chamber opening to avoid vitreous traction, but a small amount of flocculent lens material fell into the posterior segment (leading to floaters that resolved over time). The vitreous was evacuated from the anterior segment and retracted from around the zonules with irrigation, cutting, and aspiration. A second paracentesis was created to allow placement of an anterior chamber maintainer and complete lens removal. An OVD was reinstilled as necessary to support a normotensive eye. The vitrector was repositioned through the paracentesis on irrigation/aspiration/cut mode to promote the followability of the remaining cortex and allow almost instantaneous initiation of a vitrectomy by entering footpedal position 3 in case vitreous presented again.
Once the bag was free of lens material, a surprisingly large oval posterior capsular opening with fibrotic edges was observed. I dared not place a CTR and hoped that the support it would have provided would prove unnecessary because the zonulolysis was limited and small.
After careful consideration, my decision was to double capture a three-piece IOL, which was placed in the sulcus (avoiding the area of zonulolysis) through a temporal clear corneal incision. The haptics were placed in the sulcus, and the optic was captured through both the anterior capsulorhexis and the opening in the fibrotic posterior capsule. To my delight, the IOL appeared to be centered and as stable as a rock.
A 10-0 nylon, double-armed, two-bite suture was used to repair the iridodialysis, and the knot was rotated under sclera and covered by a sutured fornix-based flap. A small Siepser-style iridoplasty was performed to cover the edges of the lens optic.
After surgery, the patient’s UCVA was 20/30, and his BCVA was 20/25. A consultation with a retina specialist revealed no retinal pathology. The patient required one topical glaucoma medication to maintain a similar IOP to that in the contralateral eye. His family was counseled to beware possible progression of the traumatic glaucoma in the future. Stability was maintained for the next 6 years, at which point the patient left for college and was lost to follow-up.
1. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136-1142.
2. Jacob S, Agarwal A, Agarwal A, Agarwal A, Narasimhan S, Ashok Kumar D. Glued capsular hook: technique for fibrin glue-assisted sutureless transscleral fixation of the capsular bag in subluxated cataracts and intraocular lenses. J Cataract Refract Surg. 2014;40(12):1958-1965.
3. Jacob S, Narasimhan S, Agarwal A, Mazzotta C, Rechichi M, Agarwal A. Supracapsular glued intraocular lens in progressive subluxated cataracts: technique to retain an intact vitreous face. J Cataract Refract Surg. 2017;43(3):312-317.
4. Jacob S, Kumar DA, Rao NK. Scleral fixation of intraocular lenses. Curr Opin Ophthalmol. 2020;31(1):50-60.
5. Kumar DA, Agarwal A, Chandrasekar R, Jaganathasamy N. Iris and knot configuration after Single Pass Four Throw (SFT) pupilloplasty as imaged by the spectral-domain optical coherence tomography. Indian J Ophthalmol. 2019;67(2):209-212.
6. Rosenberg ED, Ngo V, Nattis AS. New approach to iridodialysis repair. AAO ONE Network. April 13, 2021. Accessed September 15, 2022. https://www.aao.org/clinical-video/new-approach-to-iridodialysis-repair
7. Narang P, Agarwal A. Single-pass four-throw technique for pupilloplasty. Eur J Ophthalmol. 2017;27(4):506-508.

