CASE PRESENTATION
After undergoing uncomplicated bilateral cataract surgery with an IC-8 Apthera IOL (Bausch + Lomb), a 70-year-old man presents with a desire for improved vision in his left eye. The patient’s surgical history is significant for eight-incision radial keratotomy (RK) in the right eye and 16-incision RK in the left eye.
His UCVA is 20/25 OD and 20/70 OS. His manifest refraction is -2.00 +2.00 x 101º = 20/40 OS, and his wavefront refraction is -2.50 +1.75 x 078º = 20/40 OS. A slit-lamp examination of the left eye finds 16 RK incisions and central scarring beneath Bowman membrane. The fundus appears to be normal on examination. Diagnostic imaging is shown in Figures 1 to 4.
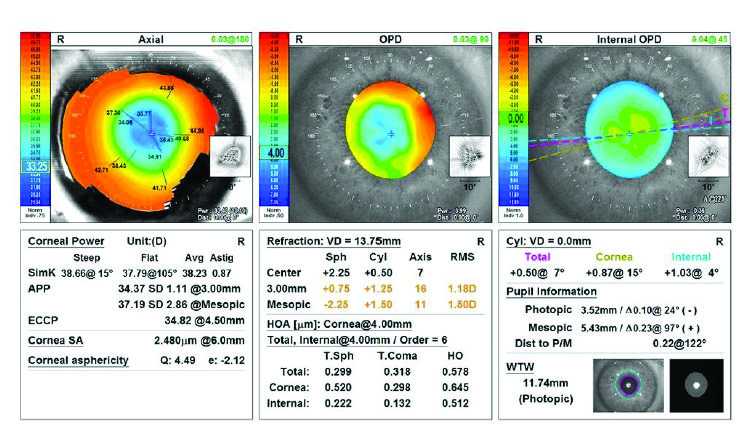
Figure 1. Topography using the OPD-Scan III.

Figure 2. Epithelial mapping.
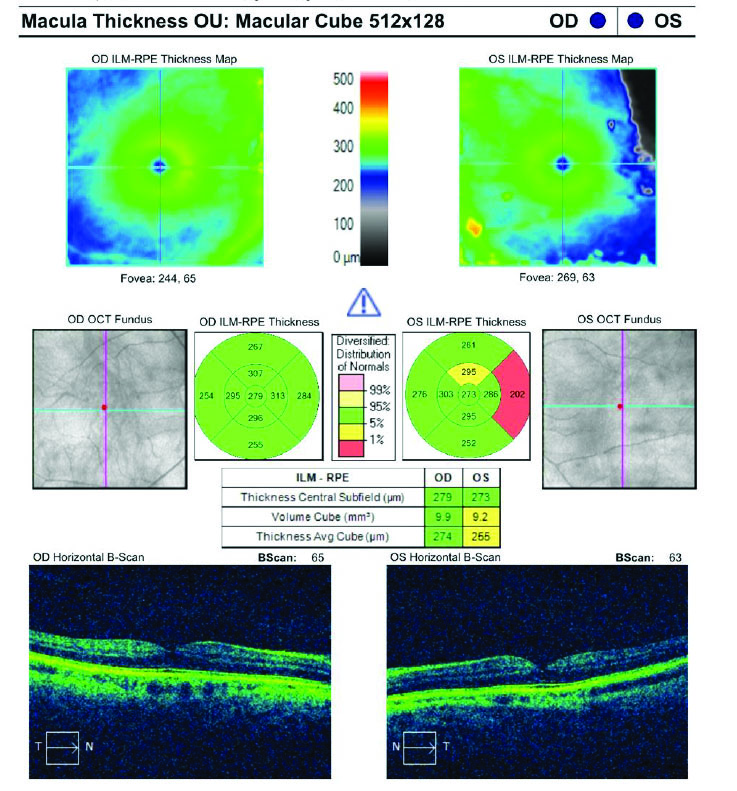
Figure 3. OCT analysis of the macula.
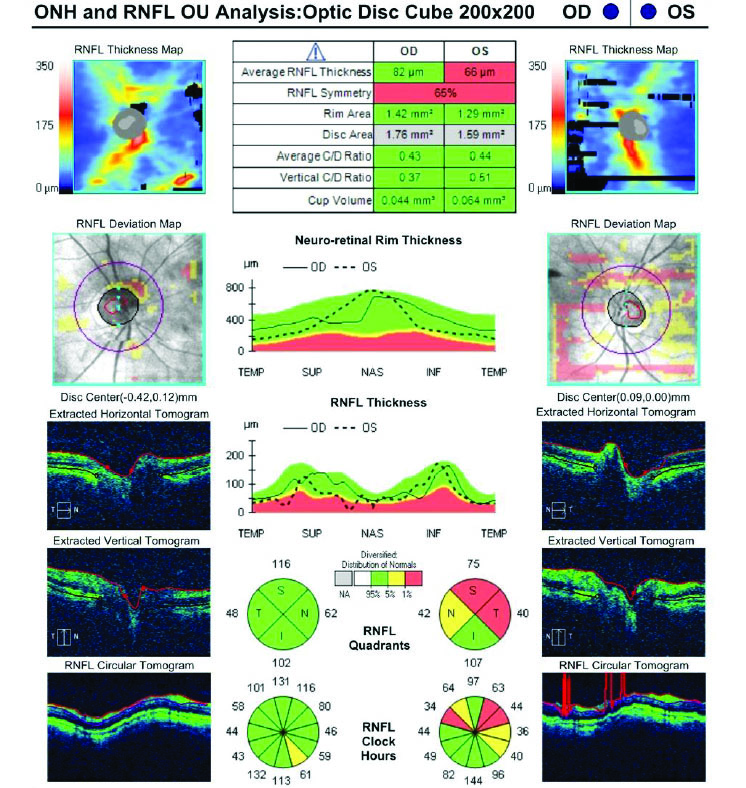
Figure 4. OCT analysis of the optic nerve.
The patient has been administering losartan 0.08% ophthalmic solution in his left eye for more than a year, which has improved his BCVA by 2 lines.
How would you proceed?
— Case prepared by Karl G. Stonecipher, MD

A. JOHN KANELLOPOULOS, MD
RK incisions, especially those that cross the limbus, create great diurnal variation. Typically, significant hyperopia in the morning decreases midday and is minimal in the evening. Depending on when the manifest refraction, which was confirmed with wavefront technology, was obtained, the 2.00 D of astigmatism in the patient’s left eye appears to be largely against the rule—a conclusion supported by the rest of the corneal imaging provided. The epithelial maps of the left eye show typical epithelial remodeling, with thickening at the flattened area in the central cornea due to the RK incisions.
The pinhole optics of the IC-8 Apthera lens can address visual symptoms—especially starbursts—in post-RK eyes. With one of these IOLs in each of the patient’s eyes, my strategy would be to treat the astigmatism in his left eye. My go-to procedure in situations like this one is surface ablation, whether wavefront-optimized or topography-guided.
The patient would be asked to conduct a contact lens trial for a couple of days. I often receive pushback from patients in similar situations, and I emphasize that the trial is important to ascertain how astigmatism correction affects their visual function throughout the day. Some of them prefer emmetropia midday, some in the morning, and some at night. The target refraction would be customized to this patient’s preference.



SIMON P. HOLLAND, MD, FRCSC, MRCP, FRCOPHTH; DAVID T.C. LIN, MD, FRCSC; AND GREG MOLONEY, MBBS (HONS), FRANZCO, FRCSC
The challenge here lies not with the treatment itself but with the diagnostic testing required to decide the best refractive outcome for the patient. He is likely hyperopic in the morning and experiences a gradual myopic shift throughout the day. The target refraction must take this shift into account and address his irregular astigmatism.
We have not had much luck with contact lens measurements during the day. We therefore perform two or three refractions at different times of day and ask patients to indicate their preference. The readings are usually consistent day-to-day but find the diurnal fluctuations troublesome. In situations like this one, the pinhole optics of an IC-8 lens generally work well.
The patient’s myopic mixed astigmatism should prove advantageous for surgical planning. The epithelial thickness maps would be used to plan transepithelial PRK.
It is surprising how many problems related to RK we still encounter, but fortunately, better ways to deal with them have become available.

ALEKSANDAR STOJANOVIC, MD, PHD, FWCRS
The optical system of the left eye is complex. The manifest refraction reflects an interplay of spherical equivalent and cylinder that is influenced by several elements:
- High positive anterior asphericity with a Q-value of +4.49 (measured by the OPD-Scan III [Nidek]) pushes the manifest refraction toward hyperopia. Correcting this oblate profile would make the eye more myopic1;
- The corneal epithelial thickness of less than 70 µm centrally and approximately 40 µm outside the 5-mm zone forms a complex epithelial lenticule that might contribute +2.00 D or more in power. Evening out the epithelium would shift the refraction toward greater myopia2;
- Irregular astigmatism, with root mean square higher-order aberrations of 0.578 μm at 4 mm, is probably reducing the patient’s corrected distance visual acuity to 20/40; and
- A coma value of 0.318 μm at 4 mm is also relatively high and may be influencing the refractive astigmatism. Without orientation data, however, the directional impact is unclear.3
Given the deep RK incisions, surface ablation is the only viable choice. Standard ablation based on the patient's manifest refraction is an option. The procedure would have to account for and preserve the effects of the aforementioned components that are shaping the manifest sphere and cylinder.
Alternatively, customized ablation could be considered, but unless reliable wavefront data can be obtained (highly unlikely here), a wavefront-guided procedure is contraindicated. Topography-guided surface ablation would be an option if reliable anterior and stromal topography data are available and all optical components can be measured precisely and accounted for, but this is also unlikely. Another option could be corneal ray tracing–guided ablation, based on high-resolution anterior, stromal, and posterior topography. Currently, this is available only with the iRes excimer laser system (iVis). Total eye ray tracing–guided ablation based on topography with the Pentacam (Oculus Optikgeräte) and Hartmann-Shack aberrometry is not suitable for highly aberrated eyes3,4 due to the Pentacam’s vulnerability for stromal opacities in posterior corneal surface topography.
The epithelium could be removed with transepithelial phototherapeutic keratectomy (PTK) or as a PTK component of transepithelial PRK, which is available on certain laser systems. The eye’s refractive profile includes a significant positive-powered epithelial lenticule, which would alter the eye’s optics unpredictably if the epithelium is removed mechanically or via alcohol. In contrast, epithelial removal by transepithelial (epithelium-on) PTK, programmed to match the maximum epithelial depth, would result in epithelial removal and partial stromal ablation and should yield a postoperative corneal surface with approximately the same anterior topography and total corneal optics as preoperatively.5
I would opt for transepithelial PTK/PRK based on the manifest refraction, with possible adjustments for diurnal variations (common in post-RK eyes). Given the inherently low predictability of outcomes in situations like this one, I would advise the patient to strongly consider nonsurgical optical correction such as spectacles or scleral contact lenses to improve his visual acuity.

WHAT I DID: KARL G. STONECIPHER, MD
After we discussed the options of glasses and scleral contact lenses, the patient elected to undergo surgery. Several refractions were obtained in the morning and evening. Attempts were made to show him his anticipated real-world postoperative vision based on those refractions. It is important to note, however, that the IC-8 Apthera lens masks astigmatism, rendering refraction challenging (click here for guidance).
Based on the patient’s favored refraction, epithelial maps, and diagnostic measurements with the Wavelight Topolyzer Vario (Alcon), PTK and PRK were performed to remove the epithelium and central scar (Figure 5). The amount of epithelial tissue removed was based on the 2- to 5-mm epithelial map (71 µm), so the total ablation was 65 µm centrally and 69 µm in the periphery. The goal was to normalize the cornea and reduce the scar to a greater extent than was achieved with losartan treatment alone.
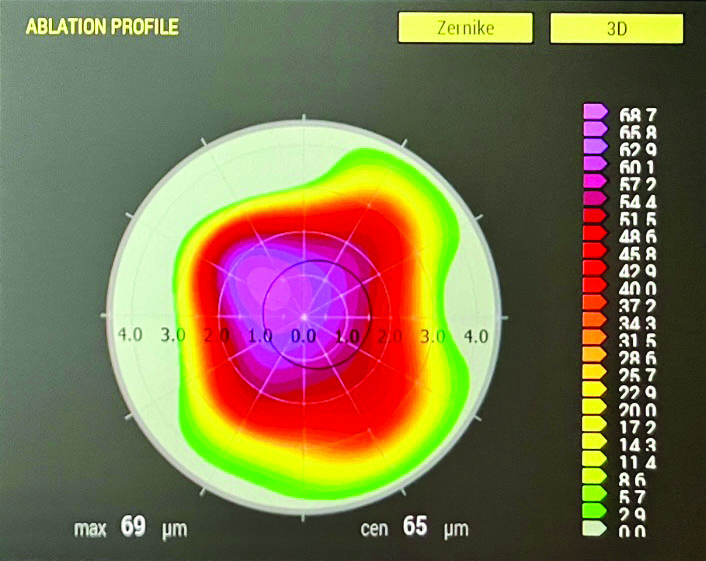
Figure 5. Ablation profile from the planned treatment.
Postoperatively, the patient’s UCVA and BCVA were 20/32 OS, and he was happy with both his quality and quantity of vision.
Dr. Stojanovic used an AI language model (GPT-5, OpenAI) to assist with language editing. All content was reviewed, verified, and revised by the article’s authors, who assume full responsibility for the accuracy and integrity of the manuscript. The AI tool was not used for data analysis, interpretation, or drawing scientific conclusions.
1. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ. Epithelial thickness in the normal cornea: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg. 2008;24(6):571-581.
2. Reinstein DZ, Gobbe M, Archer TJ, Silverman RH, Coleman DJ. Epithelial, stromal, and total corneal thickness in keratoconus: three-dimensional display with Artemis very-high frequency digital ultrasound. J Refract Surg. 2010;26(4):259-271.
3. Zhou W, Stojanovic A, Utheim TP. Assessment of refractive astigmatism and simulated therapeutic refractive surgery strategies in coma-like-aberrations-dominant corneal optics. Eye Vis (Lond). 2016;3:13.
4. Zhou W, Reinstein DZ, Archer TJ, et al. Intraoperative swept-source OCT-based corneal topography for measurement and analysis of stromal surface after epithelial removal. J Refract Surg. 2021;37(7):484-492.
5. Zhou W, Reinstein DZ, Archer TJ, et al. The impact of epithelial remodeling on surgical techniques used in topography-guided surface ablation in irregular corneas. J Refract Surg. 2022;38(8):529-537.