



It is a true honor to serve as a chief medical editor of CRST alongside my respected colleagues and dear friends Kendall E. Donaldson, MD, MS, and Cathleen M. McCabe, MD. We are grateful to our predecessors, David F. Chang, MD; Steven J. Dell, MD; John F. Doane, MD; Eric D. Donnenfeld, MD; Stephen G. Slade, MD; Robert J. Weinstock, MD; and William F. Wiley, MD, who helped build the foundation of this publication, and to the surgeon community that has trusted CRST as a forum for practical, clinically grounded exchanges.
This month’s cover series examines the surgical management of presbyopia. It seems fitting here to reflect on the past and present of this area of ophthalmology, with a primary focus on the aging crystalline lens—the root of the problem.
In 2005, Jorge L. Alió, MD, PhD, introduced the concept of optical lens dysfunction to describe continuous, age-related changes in crystalline lens clarity.1 A few years later, Daniel S. Durrie, MD; Jason E. Stahl, MD; and I helped popularize the term dysfunctional lens syndrome (DLS) as a syndromic framework for progressive lens aging.2,3 The term was intended to capture a triad of changes: declining accommodation (presbyopia), intensifying aberrations, and loss of clarity. We view the aging lens as a spectrum of dysfunction—functional, optical, and structural—rather than a single threshold event such as cataract. Harvey Carter, MD, and Dean Corbett, MD, also contributed to these early concepts.
Our perspective coincided with a shift in real-world refractive practice: more patients began seeking surgical solutions to their presbyopia. Some had a history of laser vision correction and believed their LASIK had “worn off,” when the real issue was aging of the crystalline lens. Others with emmetropic presbyopia had never needed optical correction and experienced a decline in their near visual acuity as a sudden cliff. As the demand for the surgical correction of presbyopia increased, it became clear that corneal laser strategies—though valuable in select cases—were not always the most durable approach. A lens-based solution better addressed both the refractive needs and underlying physiology of a meaningful subset of patients.
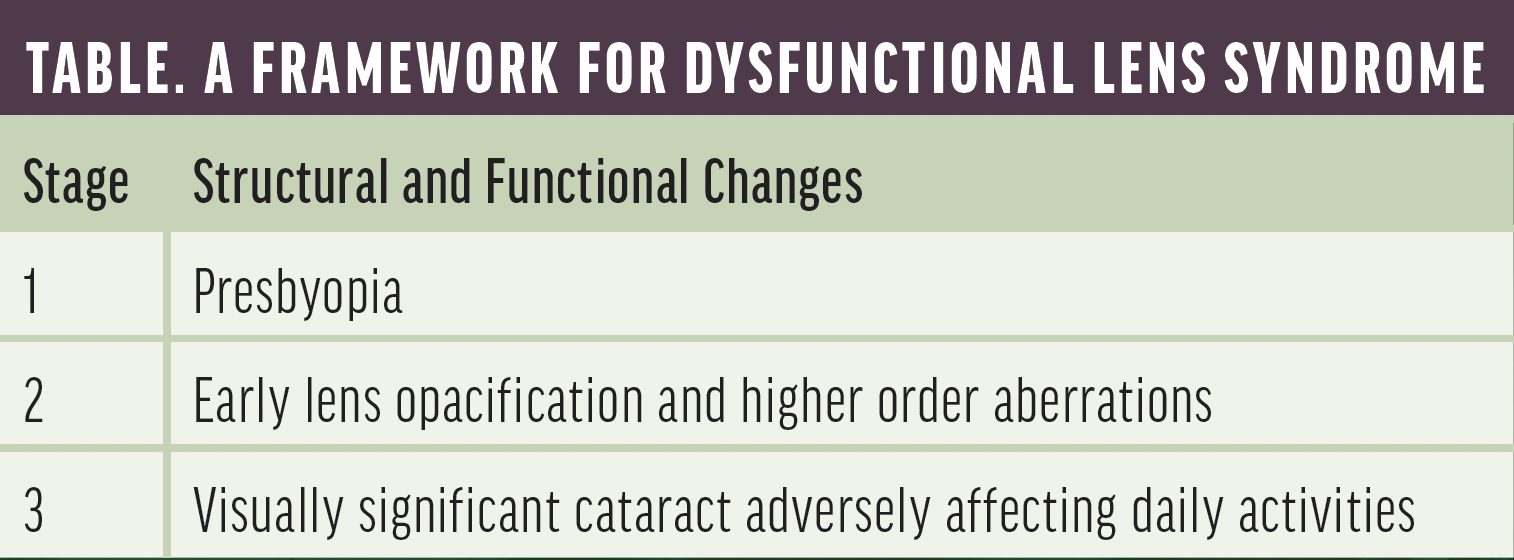
My colleagues and I published and taught these observations and introduced the DLS concept and a staged framework (Table).2 When we initially described staging and management, our general approach was to consider corneal laser vision correction strategies for stage 1, strongly consider lens-based intervention for stage 2, and perform cataract surgery to address stage 3; however, some in-betweener (eg, presbyopes with high axial myopia) may be approached differently. Our DLS framework has evolved over time, and I explore an important driver of this shift—the role of latent hyperopia as a form of DLS—in my article.
Technological advances and refinements in patient selection have led us to offer lens replacement more often—even for stage 1 DLS—in appropriately selected patients. In my practice, that recommendation is increasingly driven by the severity of presbyopic functional limitation and the patient's goals. For example, if a patient’s uncorrected near visual acuity is J6 or worse—even if their uncorrected distance visual acuity is 20/20 or better—I routinely discuss lens replacement as a primary surgical option.
Contributors to this month’s cover series address how they are thinking about lens dysfunction, how they are evaluating and educating patients, and how they are offering these procedures in a more refractive, LASIK-like workflow. Dagny Zhu, MD, discusses immediately sequential bilateral office-based lens procedures. Luke Rebenitsch, MD, and Lukas Mees, MD, address the decision-making process and updated surgical algorithms for presbyopia management. Travis Parker, MD, and Gregory Parkhurst, MD, explore the management of patients in intermediate stages of DLS. Finally, Jason E. Stahl, MD, covers the patient experience and the language of lens replacement.
George O. Waring IV, MD, FACS
Chief Medical Editor
1. Alió JL, Schimchak P, Negri HP, Montés-Micó R. Crystalline lens optical dysfunction through aging. Ophthalmology. 2005;112(11):2022-2029.
2. Waring GO IV, Rocha KM. Characterization of the dysfunctional lens syndrome and a review of the literature. Curr Ophthalmol Rep. 2018;6(4):249-255.
3. Rocha KM, Nosé W, Bottós K, Bottós J, Morimoto L, Soriano E. Higher-order aberrations of age-related cataract. J Cataract Refract Surg. 2007;33(8):1442-1446.

