




The intraoperative complications of cataract surgery involving the posterior capsule can be divided into three stages depending on the extent of vitreous travel: (1) a broken posterior capsule with an intact hyaloid membrane, (2) vitreous prolapse (Figure 1), and (3) vitreous loss.1 Vitreous prolapse is defined as vitreous advancing into the anterior segment, whereas vitreous loss is defined as vitreous violating the corneal-scleral envelope, most frequently through the incision.1 Higher stages yield a higher probability of an iatrogenic retinal tear or detachment.2
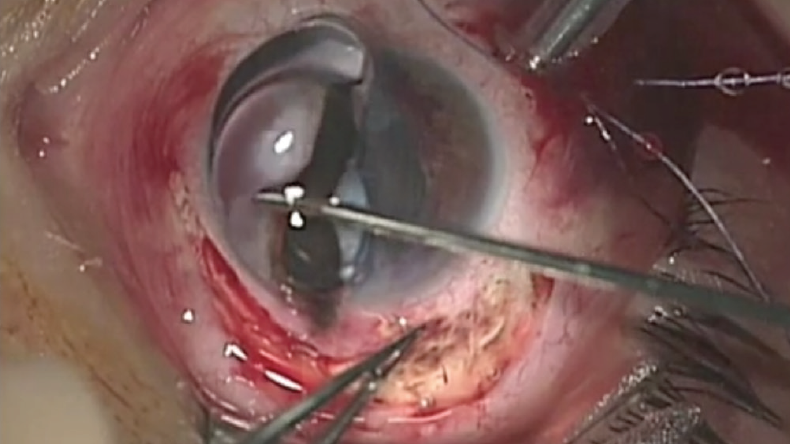
Figure 1. Vitreous prolapse occurred during surgery on an eye that had suffered a blunt ocular trauma.
Courtesy of Michele Coppola, MD, and Federico Solignani, MD
During cataract surgery, violation of the posterior capsule may cause vitreous gel to prolapse into the anterior chamber.2 According to a prospective study of 2,000 consecutive cataract extractions, posterior capsular rupture (PCR) without vitreous loss occurred in 0.16% of patients, and PCR with vitreous loss occurred in 0.53% of patients.3
It is imperative to identify a vitreous event (prolapse or loss) in a timely manner and to respond appropriately in order to prevent sight-threatening complications.
CONSIDERATIONS
Risk factors. A patient’s preoperative risk factors for PCR and a detailed history should be assessed preoperatively so that appropriate precautionary measures may be taken. Risk factors warranting consideration include a dense cataract, transillumination iris defects, phacodonesis, complicated cataract surgery in the fellow eye, marked ametropia, floppy iris syndrome, pseudoexfoliation, prior vitrectomy, advanced age, and a posterior polar cataract.1
Anatomical considerations that may result in vitreous loss without PCR should also be evaluated preoperatively. These include lens subluxation, coloboma, and a history of ocular trauma.
Prevention. Potential precautionary measures include peribulbar anesthesia, keeping vitrectomy instrumentation on standby, booking additional time for complex cases, and having backup implants on hand.1
Signs. Warning signs of a PCR are plentiful and include the following2:
- An asymmetrically enlarged pupil with remote movement of the iris when the incision is touched;
- A sudden deepening of the anterior chamber;
- A sudden pupillary bounce or change in pupil size;
- An inability of lens particles to migrate to the phaco needle during phacoemulsification;
- The sinking of lens material into the back of the eye;
- Spidering of the posterior capsule;
- Tilting of the nuclear equator; and
- The surgeon’s inability to rotate a previously mobile nucleus.
Management. Intervention varies based on the severity of vitreous migration, but initial steps to prevent further complications and assess the situation are similar. Although a natural response is to withdraw instrumentation immediately, this maneuver can cause the pressure in the anterior chamber to drop suddenly, potentially leading to an extension of the capsular tear, anterior suction of the vitreous, and extrusion of vitreous through the incision along with the instrument as it is extracted. The steps described in Prevent Further Complications and depicted in Figure 2 are a better alternative.1
Prevent Further Complications
No. 1. Pause and take a deep breath. Nothing happens if nothing changes.
No. 2. Without withdrawing the phaco instrument, go to footpedal position 1. Stop phacoemulsification and aspiration.
No. 3. Maintain chamber stability. Do not allow collapse.
No. 4. Through the sideport incision, fill the anterior chamber with enough of a dispersive OVD to close the incision sufficiently as the phaco tip is withdrawn.
No. 5. Assess the situation and the extent of vitreous travel.
No. 6. Proceed based on severity (detailed below).
- Intact anterior hyaloid and broken posterior capsule. A dispersive OVD is carefully placed over the posterior capsular tear, and a cohesive OVD is instilled in Berger space to create an additional barrier to the anterior hyaloid membrane. Some surgeons recommend performing a posterior capsulorhexis to prevent the tear from spreading radially.1
- Vitreous prolapse. The phaco probe is kept in place while a dispersive OVD is injected through the sideport incision in an effort to maintain a more stable pressure gradient, support the anterior chamber anatomy, and create an additional barrier between the vitreous and the lens. The phaco tip may then be removed to check for vitreous loss, and a vitrectomy may be performed if warranted.1
- Vitreous loss. The same procedure described for vitreous prolapse should be employed, but extra care is required. Broad sweeping and techniques using a Weck-Cel sponge (Beaver-Visitec International) should be avoided because they can place undue traction on the vitreous and result in a retinal tear or detachment. Staining the capsule with trypan blue dye (Figure 2 in the article) or triamcinolone acetonide (Triesence, Alcon) can facilitate visualization of the vitreous.1
1. Shareef S, Arbisser LB. Cataract extraction requiring vitrectomy due to violation of the posterior capsule with lens implantation (optic capture, in the bag, sulcus, and ACIOL). In: Rosenberg E, Nattis A, Nattis R, eds. Operative Dictations in Ophthalmology. Springer; 2020:215-235.
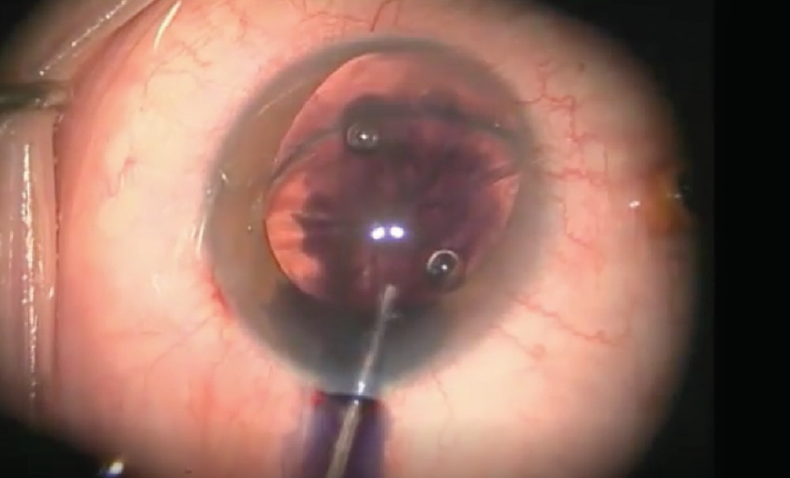
Figure 2. Trypan blue dye is instilled in the eye.
Courtesy of Michael E. Snyder, MD
VITRECTOMY
Whether it is more beneficial for anterior segment surgeons to perform a vitrectomy via a pars plana or a limbal anterior approach is a subject of debate.4
Pars plana vitrectomy. Minimal traction should be placed on the vitreous base. Vitreous follows a pressure gradient from high to low. It is therefore ideal to create the lower-pressure environment in the posterior segment, which can only be accomplished via pars plana vitrectomy (PPV).
Working closer to the vitreous base and amputating the gel in the posterior segment also directs the vitreous toward the base rather than the corneal incision. Additionally, calling the vitreous backward may help to eliminate the use of a sweeping technique from the sideport and avoid excessive traction through the pupil.1 A PPV may minimize zonular tension on an already compromised system from instrument positioning and vitreous course. Additional advantages include decreased operative time, greater patient comfort, reduced conjunctival scarring, a lower rate of infection, and fewer complications.2 PPV is our preferred method of management.
One of the greatest risks for anterior segment surgeons performing PPV is the creation of retinal tears and detachment.5 In a single-surgeon, retrospective observational case series examining 415 eyes, retinal breaks were found in 48 (11.6%), with nine (2.2%) resulting in retinal detachment.6
This complication can occur when an instrument engages the vitreous base or when a microvitreoretinal blade rather than a trocar system is used to create a scleral opening.5
After PPV, it is prudent to check the periphery for retinal tears and holes.
Limbal anterior vitrectomy. The advantages of performing a PPV rather than a limbal anterior vitrectomy center on creating a low-pressure environment in the posterior chamber to reduce traction on the vitreous and lower the probability of a retinal tear or detachment. Similar advantages can be realized with an anterior approach if the following techniques are used:
- The cutting port of the aspirating handpiece is placed behind the posterior capsular opening to create a low-pressure environment posteriorly and reduce traction on the anterior vitreous;
- Bimanual vitrectomy instruments with separated I/A and cutting ports are used; and
- Small watertight paracenteses for the vitrectomy probes are created to prevent wound leaks from bringing the vitreous forward.2
A limbal anterior approach may cause endothelial damage secondary to turbulent flow, which is not encountered during PPV. Additionally, direct contact with the cutter can damage the iris and capsule.1 Finally, residual vitreous strands may be challenging to remove and may not become apparent until the day after surgery.
CONCLUDING SURGERY AND POSTOPERATIVE CARE
After cataract surgery with vitrectomy, the capsule can be stained with triamcinolone acetonide to allow the surgeon to look for incarcerated vitreous. Watertight closure of the main wound can be accomplished with a 10-0 nylon interrupted or mattress suture and stromal hydration. Acetylcholine (Miochol-E, Bausch + Lomb) or carbachol intraocular solution (Miostat, Alcon) can be instilled in the eye to induce pupillary miosis. This protects the IOL position, further compartmentalizes residual vitreous present in the posterior chamber and vitreous cavity, and helps to identify residual vitreous strands, which present as peaking of the pupillary sphincter. Intravenous administration of acetazolamide (Diamox, Duramed Pharmaceuticals) can help to prevent a postoperative IOP spike if a residual amount of an OVD is present.2
Due to the combination of ocular surface bacteria contaminating the aqueous humor in 7% to 43% of cataract operations and the relatively high turnover rate of aqueous humor (100 min) compared to the vitreous humor that does not regenerate, inadvertent breaks in the capsule increase the risk of endophthalmitis 14-fold.7 Intracameral and subconjunctival antibiotics may be prophylactically administered; the ESCRS demonstrated that one dose of 1 mg in 0.1 mL of intracameral cefuroxime administered at the conclusion of surgery reduced the incidence of endophthalmitis by a factor of 5, from 0.34% to 0.07%.8
The eye should be inspected for vitreous in the anterior chamber; peaking of the pupil, which can indicate recurrent vitreous loss or prolapse; retained anterior capsular flaps; an IOL loop entrapping the iris from the posterior surface; and dehiscence of the cataract surgical wound with iris prolapse.8 A Seidel test should be performed to check for leaks from the cornea, sclera, and conjunctiva.9 To prevent cystoid macular edema, NSAID or steroid drops should be administered for a minimum of 6 weeks.
A retinal examination and OCT imaging should be performed within 2 weeks to look for retinal holes, tears, and detachment. These patients are at increased risk of developing glaucoma and retinal complications. It is therefore important that they know to contact their eye care provider immediately if they experience acute eye pain or decreased vision.1
CONCLUSION
Learning how to identify a vitreous event and responding appropriately can help to prevent sight-threatening complications during cataract surgery. Intervention will vary based on the severity of the event, but one must avoid the natural response to withdraw instrumentation immediately. The best reaction is to pause, take a deep breath and then proceed with the methods of management described in this article.
1. Arbisser LB. Comprehensive strategies for unplanned vitrectomy for the anterior segment surgeon. Accessed March 22, 2021. Cataract & Refractive Surgery Today. 2012;1(suppl):3-20.
2. Shareef S, Arbisser LB. Cataract extraction requiring vitrectomy due to violation of the posterior capsule with lens implantation (optic capture, in the bag, sulcus, and ACIOL). In: Rosenberg E, Nattis A, Nattis R, eds. Operative Dictations in Ophthalmology. Springer; 2020:215-235.
3. Misra A, Burton RL. Incidence of intraoperative complications during phacoemulsification in vitrectomized and nonvitrectomized eyes: prospective study. J Cataract Refract Surg. 2005;31(5):1011-1014.
4. Thornton IL, McMains BK, Snyder ME. Long-term safety and efficacy of single-port pars plana anterior vitrectomy with limbal infusion during anterior segment surgery. J Cataract Refract Surg. 2018;44(7):878-883.
5. Arbisser LB. Pars plana anterior vitrectomy for the anterior segment surgeon. In: Chakrabarti A, ed. Posterior Capsular Rent. Springer; 2017.
6. Moore JK, Kitchens JW, Smiddy WE, Mavrofrides EC, Gregorio G. Retinal breaks observed during pars plana vitrectomy. Am J Ophthalmol. 2007;144(1):32-36.
7. Durand ML. Endophthalmitis. Clin Microbiol Infect. 2013;19(3):227-234.
8. Bellucci R, Busin M, Vajpayee R. Peaked pupil. Cataract & Refractive Surgery Today Europe. 2007;2(1). Accessed March 22, 2021. https://crstodayeurope.com/articles/2007-jan/0107_08-php/#:~:text=Pupil%20distortion%20after%20cataract%20surgery,surgical%20wound%20with%20iris%20prolapse
9. Endophthalmitis Study Group, European Society of Cataract & Refractive Surgeons. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg. 2007;33(6):978-988.

