



Pars plana vitrectomy (PPV) is a well-recognized risk factor for cataract progression. In almost all cases, a visually significant cataract develops months to years after surgery. Rarely, a cataract develops 1 to 7 days after a vitreous procedure. The cause of this acute, rapidly progressive cataract is frequently blunt or penetrating trauma to the posterior capsule (PC) caused by PPV instrumentation, the needle of an intravitreal injection, or even an Nd:YAG vitreolysis performed for floaters.
GRADUAL CATARACT
The increased risk of performing cataract surgery on an eye with a history of vitrectomy or injection is well documented. After PPV, for instance, the risk of zonular dialysis (1.3% vs 0.6%) and dropped nuclear fragments (0.6% vs 0.2% P < .0001) but not posterior capsular rupture (PCR) increases.1 The zonules can be inconspicuously damaged by PPV instruments and/or an irrigation cannula. A PCR can rapidly lead to the posterior dislocation of lens fragments in a vitrectomized eye compared to one with the cushioning from vitreous.
Intravitreal injections have also been implicated in an increased incidence of PCR. Shalchi et al found an odds ratio of 1.66 after an intravitreal injection,2 and Lee et al found that a PCR was 2.59 times more likely to occur after 10 intravitreal injections.3 Hahn et al reported an increased rate of acute- and delayed-onset endophthalmitis in eyes that had received intravitreal injections.4
SUDDEN-ONSET CATARACT
When a patient presents with a rapidly progressive cortical and then white cataract a few days after a vitreous procedure, the cataract surgeon should proceed with caution. A rupture or breach of the PC must be assumed, even though a capsular contusion can also be causative. Hydration of the crystalline lens creates rapidly progressive whitening. Frequently, a PC opacity, opening, or plaque can be visualized at the slit lamp before the lens becomes completely opaque.
A few helpful pearls for treating these types of acute cataracts are as follows.
No. 1: Thorough informed consent is important. This discussion should take place at the outset of the patient’s care. It should describe the risks of intervention, the possibility of deferring a premium IOL in certain intraoperative scenarios, and the potential need for subsequent surgery.
No. 2: Schedule these surgeries with care. I operate on eyes with rapidly progressive cataracts at the hospital on a day when my retina colleague also has time blocked in another room.
No. 3: Note the location, size, and shape of the capsular breach on slit-lamp examination. As long as there is no significant inflammation, it is advisable to observe these patients for up to 4 to 6 weeks before proceeding with surgery. This delay allows PPV-related air and gas to be resorbed and, more importantly, a fibrous plaque to develop on the PC. This plaque acts to plug the PC defect or at least discourage it from extending during cataract extraction (Figure 1).
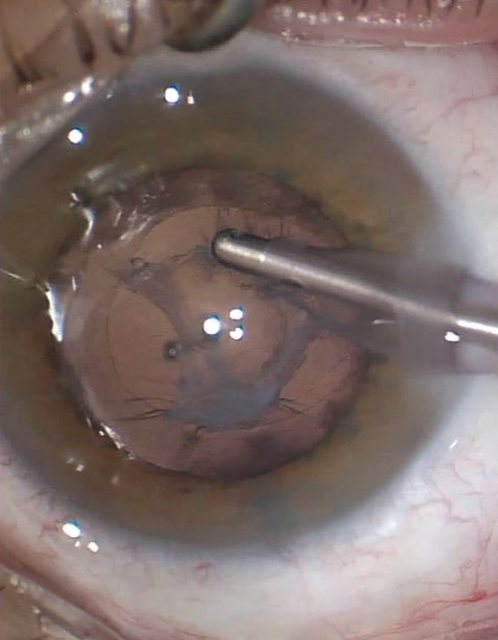
Figure 1. A protective posterior capsular plaque has formed around a PC defect in this post-PPV eye with an acute cataract. The IOL is placed in the bag, and an Nd:YAG laser can be performed at a later date.
SURGICAL APPROACH
A sudden-onset cataract should be treated similarly to a posterior polar cataract. (Scan the QR code now to watch a related surgical case.) I recommend creating a 5.0- to 5.2-mm capsulotomy, whether manually or with a femtosecond laser, to allow easy prolapse of the crystalline lens and provide adequate capsular support for a sulcus-fixated IOL with optic capture if necessary (Figure 2). Staining of the capsule with trypan blue dye is frequently helpful.
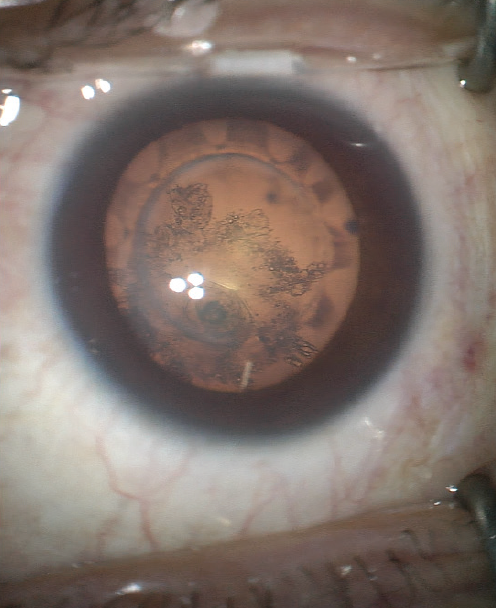
Figure 2. A laser capsulotomy was created in an eye that had previously undergone an Nd:YAG vitreolysis for floaters. A PC breach led to the sudden formation of a cataract. The laser created a well-centered, 5.2-mm capsulotomy should sulcus fixation of an IOL with optic capture be required.
I avoid hydrodissection and instead perform slow, well-visualized hydrodelineation. The endonucleus can then be emulsified. I prefer a supracapsular technique to minimize zonular forces. Careful refilling of the anterior chamber with OVD helps to prevent shallowing during instrument withdrawal.
The I/A tip can be used to slowly remove the epinuclear plate followed by the cortex; the affected area should be removed last. If the PC is intact and a thin fibrous plaque is noted, I elect to leave it in place for a subsequent Nd:YAG laser capsulotomy. A one-piece acrylic hydrophobic IOL, including toric or presbyopia-correcting designs, if indicated, can then be placed in the bag.
If an opening in the PC is noted, a dispersive OVD is placed in the area to act as a barrier. Typically, the breach will not extend, and a decision about in-the-bag placement of the IOL is made based on the size and location of the opening. If posterior capsular support is deemed insufficient, a three-piece IOL should be placed in the sulcus with optic capture.
The case concludes with the intravitreal administration of antibiotics (eg, moxifloxacin), and the postoperative drug regimen includes a combination of steroids and NSAIDs for prophylaxis against cystoid macular edema.
CONCLUSION
The sudden onset of a cataract after vitrectomy and intravitreal injection can be upsetting for patients. With proper technique, informed consent, and contingency planning (see Key Points), the anterior segment surgeon is well equipped to handle these challenging cases.
Key Points
- Presuming that the posterior capsule has been breached, a cataract develops rapidly after vitrectomy or an intravitreal injection.
- Allow 4 to 6 weeks, if possible, for a fibrous plaque to seal off the posterior capsular defect.
- Approach an acute cataract as you would a posterior polar cataract.
- Perform hydrodelineation instead of hydrodissection.
- If a premium IOL is planned, counsel the patient that an alternative IOL may be implanted instead.
- Use intracameral antibiotics such as moxifloxacin in these high-risk eyes.
1. Soliman MK, Hardin JS, Jawed F, et al. A database study of visual outcomes and intraoperative complications of postvitrectomy cataract surgery. Ophthalmology. 2018;125(11):1683-1691.
2. Shalchi Z, Okada M, Whiting C, Hamilton R. Risk of posterior capsule rupture during cataract surgery in eyes with previous intravitreal injections. Am J Ophthalmol. 2017;177:77-80.
3. Lee AY, Day AC, Egan C, et al; United Kingdom Age-related Macular Degeneration and Diabetic Retinopathy Electronic Medical Records Users Group. Previous intravitreal therapy is associated with increased risk of posterior capsule rupture during cataract surgery. Ophthalmology. 2016;123(6):1252-1256.
4. Hahn P, Yashkin AP, Sloan FA. Effect of prior anti-VEGF injections on the risk of retained lens fragments and endophthalmitis after cataract surgery in the elderly. Ophthalmology. 2016;123(2):309-315.

