

Several years ago, I began using my femtosecond laser system instead of a blade for creating arcuate corneal incisions to manage astigmatism. Laser incisions have more consistent parameters than those made with a blade.1 What remains the same is that a deeper, longer, and more centrally located incision reduces astigmatism to a greater degree.
NOMOGRAMS
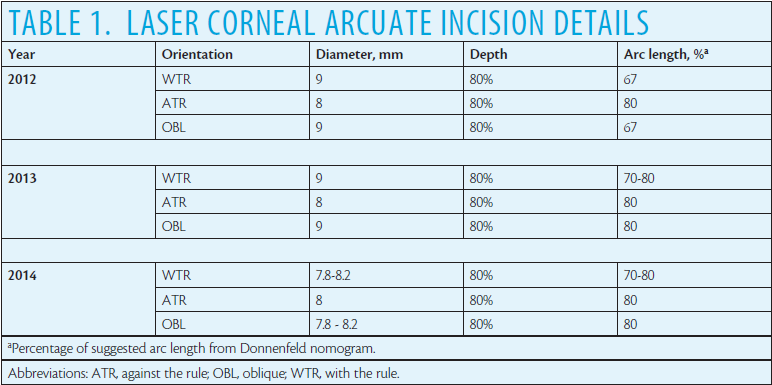
Laser arcuate incision parameters are often determined using standard nomograms intended for limbal relaxing incisions (LRIs) made with a blade. I myself started with a standard nomogram; the arc length I used was specified as a percentage of the arc length suggested by the Donnenfeld nomogram for manual LRI planning.2 Table 1 shows my original (2012) adjustment factors and the changes I made over the years.
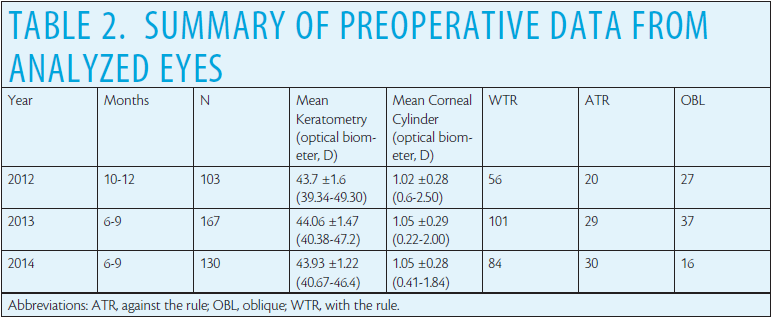
Surgeons in the clinic where I practice use the LenSx Laser (Alcon) to perform all arcuate incisions. I evaluated clinical records from a 3- to 4-month period in each of the years 2012, 2013, and 2014. Cases with surgical or postoperative complications were excluded. More than 100 eyes were available for analysis from each of the time periods reviewed. Table 2 shows the general characteristics of these eyes. There was no statistically significant difference in the mean preoperative keratometry (P = .13), the mean preoperative corneal astigmatism (P = .70), or the distribution of astigmatism orientation by year (chi-square test, P = .39). In all 3 years, the mean preoperative corneal astigmatism was not clinically significantly higher for any given orientation (< 0.25 D in all cases).
I analyzed postoperative refractive astigmatism during a 2-year period, with attention to the preoperative orientation of corneal astigmatism, to document how incremental changes in the length and location of the incision influenced the amount of residual refractive astigmatism. I categorized my outcomes by orientation, because I believe that the orientation of the anterior corneal astigmatism is an important factor in the effectiveness of arcuate incisions.
RESULTS
The results described herein are based on changes I made after examining outcomes for a given year; laser incision planning for 2013, for instance, was based on an analysis of refractive outcomes from 2012. The subsequent changes I made were incremental. Table 2 shows the summary results for the data I analyzed. Astigmatism was considered with the rule (WTR) if the steep meridian was oriented within 20º of vertical (ie, 70º-110º) and against the rule (ATR) if the steep meridian was oriented within 20º of horizontal (ie, 0º-20º or 160º-180º); eyes not classified as WTR or ATR were classified as oblique (OBL).
As Figure 1 shows, my analysis of my 2012 results bore out my suspicion that there were differences in effect with orientation. The algorithm I was using for WTR corneas was highly accurate, whereas my results with ATR and OBL corneas showed significantly higher residual astigmatism. A review of the orientation of the residual refractive astigmatism indicated an undercorrection in all cases, though with more variability in the ATR cases. Undercorrection with laser arcuate incisions has been documented.3,4
Perhaps more important, the percentage of patients with postoperative cylinder of 0.50 D or less was statistically significantly higher in the WTR group (52/56 or 93%) than in the OBL group (16/27 or 59%; P < .01) and the ATR group (15/20 or 75%; P = .05). On the basis of the 2012 results, I increased the amount of OBL correction in 2013. I also raised the amount of WTR correction but to a lesser extent than the OBL correction, as shown in Table 1.
INCREMENTAL CHANGES
In 2013, I made incremental changes to the incision’s arc length, followed by changes to the incision’s diameter in 2014. All changes were specific to the orientation of the measured anterior corneal astigmatism.
Increasing the arc length left more eyes in the OBL group with residual astigmatism of 0.50 D or less in 2013 than in 2012 (29/37 [78%] vs 16/27 [59%]; P < .01). This change (Figure 2) was not statistically significant (P = .08), however, this was likely due to the small number of cases.
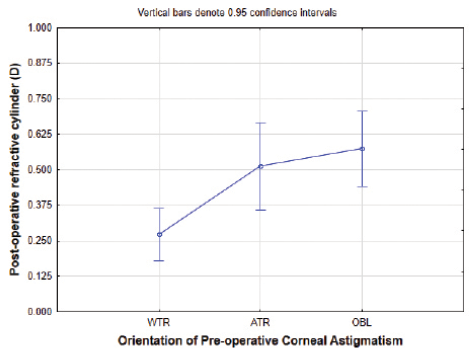
Figure 1. Residual refractive astigmatism by corneal astigmatism orientation in 2012.
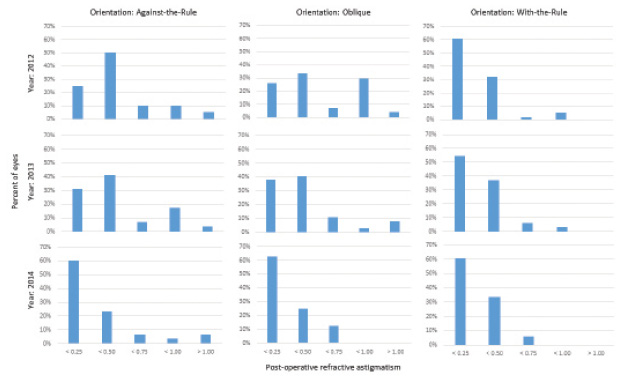
Figure 2. Postoperative astigmatism by year and orientation.
FURTHER IMPROVEMENT
I felt that I could further improve my results. I observed that, when docking the eye to the laser, a slight tilt did not allow proper positioning of some of the arcuate incisions. One incision would be tilted a little more into the cornea, and the other one a little farther out toward the limbus. To avoid this potential source of error, I manually reduced the incision’s diameter for WTR and OBL orientations (which were not changed in 2013) from 9 mm to between 7.8 and 8.2 mm in 2014. The arc length is automatically shortened by the laser system’s software in these cases; the smaller arc length at the smaller diameter has the same effect as a larger arc at 9 mm. The advantage of reducing the diameter was a more centrally located incision, though it remained outside the patient’s dilated pupil. The more central placement reduced the perceived effect of slight eye tilt, and it allowed better visualization and hence more accurate localization of the arcuate incision.
The sequential changes to the arc length in 2013, followed by the diameter in 2014, significantly improved my results in eyes with OBL anterior astigmatism. The number of eyes with less than 0.25 D of residual refractive astigmatism increased from 25% in 2012 to 38% in 2013 and 62% in 2014. The WTR category included the highest number of patients and the lowest postoperative astigmatism in 2012, so incremental improvement was minimal. The variability in the ATR results makes understanding the improvement associated with this orientation less clear. As seen in Figure 2, the residual refractive astigmatism and the percentage of eyes with 0.50 D or less of postoperative refractive astigmatism in 2014 were not statistically significantly different between the anterior corneal astigmatism orientation groups.
The mean refractive cylinder for all eyes in 2014 was 0.27 ±0.29 D. My 2014 results were statistically significantly better than my results in 2012. Refractive cylinder was significantly lower, with less variability, than that reported for LRIs made with a blade (0.56 ±0.87 D)5 or laser arcuate incisions using standard nomograms (0.33 ±0.42 D in one study4 and 0.55 ±0.40 D in another3). My 2014 results appear similar to those reported in patients receiving toric IOLs. In one study, patients had mean preoperative corneal astigmatism of 1.06 D, similar to my results, with mean postoperative refractive astigmatism of 0.31 D after toric IOL implantation. In that same toric IOL study, 92% (170/185) of eyes had 0.50 D of refractive astigmatism or less after surgery.6 Similarly, 91% (118/130) of eyes I treated in 2014 had 0.50 D of refractive astigmatism or less postoperatively. This finding confirms the increased benefit I have observed with laser arcuate incisions versus manual LRIs after adjusting the standard nomogram based on the orientation of the preoperative anterior corneal astigmatism.
CONCLUSION
Clinical outcomes with laser arcuate incisions can benefit from a personal customization of the algorithm. I addressed a systematic undercorrection of eyes with OBL corneal astigmatism by increasing the incision’s arc length and decreasing its diameter. The standard nomogram was effective for WTR astigmatism, so only a minor adjustment was required.
Analyzing postoperative refractive astigmatism based on the orientation of the anterior corneal astigmatism is useful. Surgeons who do not adjust their nomograms may be limiting their potential for improved results with laser technology.
1. Mastropasqua L, Toto L, Mastropasqua A, et al. Femtosecond laser versus manual clear corneal incision in cataract surgery. J Refract Surg. 2014;30:27-33.
2. Abbott Laboratories. Welcome to the AMO LRI calculator software website. http://www.lricalculator.com. Published 2010. Accessed June 4, 2015.
3. Venter J, Blumenfeld R, Schallhorn S, Pelouskova M. Nonpenetrating femtosecond laser intrastromal astigmatic keratotomy in patients with mixed astigmatism after previous refractive surgery. J Refract Surg. 2013;29:180-186.
4. Rückl T, Dexl AK, Bachernegg A, et al. Femtosecond laser-assisted intrastromal arcuate keratotomy to reduce corneal astigmatism. J Cataract Refract Surg. 2013;39:528-538.
5. Ouchi M, Kinoshita S. Prospective randomized trial of limbal relaxing incisions combined with microincision cataract surgery. J Refract Surg. 2010;26:594-599.
6. Ernest P, Potvin R. Effects of preoperative corneal astigmatism orientation on results with a low-cylinder-power toric intraocular lens. J Cataract Refract Surg. 2011;37:727-732.
Paul Ernest, MD
• TLC Eyecare and Laser Centers, Jackson, Mississippi
• paul.ernest@tlceyecare.com
• financial disclosure: financial support for this investigator-initiated study was provided by Alcon; no financial or proprietary interest in any product, method, or material mentioned was acknowledged

