
Visit other practices, and host visitors at yours!

BY WILLIAM F. WILEY, MD
I look back at my ophthalmic knowledge foundation and see that it was built on the education I received during residency. I trained just over 10 years ago, and at that time, in residency, we learned through multiple channels: attending physicians, senior residents, studying for examinations, and/or preparing for presentations. I remember, throughout my training, referring to multiple written sources. These included textbooks (Albert and Jakobiac was a favorite), the American Academy of Ophthalmology’s Basic and Clinical Science Course, the mainstay monthly ophthalmic journals (the “blue” journal, the “orange” journal, etc.), and the occasional “throw-away” publication. All of these sources, from personal interactions to the written works, were crucial to helping me build the basics of my ophthalmic knowledge. Since my residency, however, there have been numerous breakthroughs in ophthalmic techniques, technology, and understanding. These have also coincided with a functional paradigm shift in the technology available for creating, sharing, and consuming information.
Once looked down upon, the so-called throw-aways are now immortalized in the digital age. “Speed to print” has become extremely important for the sharing of knowledge; periodicals have proven successful at gathering, publishing, and distributing information in a highly efficient and timely manner. Their online accessibility and searchability have greatly increased their value. The ability to cross-reference articles through smart links and incorporate video with authors’ commentary has further increased their power. MillennialEYE is one example of an app-based resource.
RECORDED CASES
In residency, I remember recording one of my early extracapsular cataract videos on VHS. The case turned out pretty well, and the tape was reviewed multiple times by subsequent residents. The tape was handed from resident to resident, sometimes being left at home or other times being left in an old machine. Ultimately, the tape was lost or destroyed. Now, with tools like Eyetube.net and YouTube, video can be recorded and immediately shared around the world. With instant access to new surgical techniques, these sites allow surgeons to absorb, improve, and innovate the surgical process in a much quicker and more effective manner. Furthermore, there has been an increase in the quality of recording, with three-dimensional microscopes and video playback, allowing observing surgeons to view recorded video in three dimensions and have an experience akin to performing the surgery. This type of technology and experience can help speed up the learning curve for new technology and techniques. Video has always been one of the highlights at the major and boutique meetings. With improvements in quality, dimension, and experience, these meetings are more valuable with the advanced video presentations.
SMARTPHONE
The smartphone has allowed for better and faster learning through multiple avenues. The ability to text colleagues and ask a quick question in the middle of a surgery day has allowed me to share basic knowledge in an efficient manner. There are occasions when a colleague will ask: “What are your latest settings on the femtosecond laser?” A quick and easy response is simply to snap a picture with my phone and text the answer within minutes. Email listservs can be quickly accessed on the phone. During my downtime at the office, I find myself browsing the e-mail listservs/blog services and reading questions posted by ophthalmologists with often long and passionate responses from other experienced physicians. Google at my fingertips 24/7 gives me almost unlimited access to answers, and it is a great starting point for locating a number of resources. What used to take me hours via trips to the library I can do in minutes on my cell phone from nearly anywhere. Numerous reference-type apps allow me to access core knowledge, information on pharmaceuticals, videos, and more.
VISITING OTHER PRACTICES
Another way I learn is through traveling to other practices and hosting visitors at my colleagues’ and my practice. With multiple options for expensive equipment, it is nearly imperative to observe equipment in action prior to purchase. I traveled to multiple locations in the United States and abroad before making a final decision on a femtosecond laser for cataract surgery. With machines costing more than $500,000, I wanted to make sure our practice was making the proper investment. During these office visits, I learned more than what I set out to originally. Surgical technique, patient flow, and patients’ experiences are all better seen in person rather than reading about them in print.
Visitors to our office often leave thinking about buying another piece of technology that we use in addition to the main technology they were interested in. Furthermore, hosting visitors is a two-way street. Every time I host a visiting surgeon, I learn at least one thing that our center could improve. If it is important to attend at least one major ophthalmic meeting a year, I would argue it may be equally important to visit at least one practice per year to absorb valuable pearls in person.
CONCLUSION
The key to learning and advancing my knowledge is through communication with my peers. In the past, most of this interaction may have been through the written word on paper. Now, technology has allowed communication to travel faster and at a higher level of sophistication through the various modes of technology available.
Surf the Web, but attend the meetings.

By Elizabeth Yeu, MD
Thank goodness that the learning process is an evolving one that does not stop after residency. Beyond the format of formal residency and cornea fellowship training, however, I love being able to focus on what I want to learn, which often involves new technologies and surgical techniques in the dynamic anterior segment subspecialty. Such information is readily available through various virtual portals and websites, but when it comes to meetings, I am there in the flesh.
INTERNET RESOURCES
For a very specific technique or question (eg, Descemet membrane endothelial keratoplasty techniques or mentalis muscle Botox injection [onabotulinumtoxinA; Allergan] to reduce chin dimpling), I search Google, Eyetube.net, or YouTube. I find that these websites provide high-yield videos that often highlight the key points of the procedure of interest. More importantly, I enjoy listening to the narration, because it reveals nuances and points out pearls specific to that particular step.
I also like the Video Atlas that Thomas Oetting, MD, has compiled for the University of Iowa’s eyerounds.org website at http://bit.ly/1GxC74G. The atlas offers a broad array of excellent videos demonstrating both basic and advanced cataract surgical techniques such as the fishtail insertion of capsular tension rings. Moreover, this website includes videos covering the different subspecialties of ophthalmology.
In addition to surgical videos, I value any resource that supports perioperative management. For example, I felt very prepared to perform my first surgeries with the iStent Trabecular Micro-Bypass Stent (Glaukos) after completing the online training course and wet lab as well as several cases with a surgical representative in the OR. It has been webinars, trade journal articles, and, more recently, weekly emails from the company, however, that provided me with essential, experience-based pearls for successful outcomes.
MEETINGS
I much prefer to attend meetings physically as opposed to virtually, an option for some large conferences. I usually pick up the most useful cataract surgical tips during video-based sessions involving a panel of experts. User meeting groups are another wonderful forum. For example, LenSx Laser user meetings (Alcon) have played a huge role in the successful incorporation of laser cataract surgery into my refractive surgery practice, both clinically and administratively. Also beneficial have been the focused educational sections at small meetings such as the AECOS Summer Symposium (American-European Congress of Ophthalmic Surgery) as well as the subspecialty days that precede the annual meetings of the American Academy of Ophthalmology and the American Society of Cataract and Refractive Surgery.
An advantage of physically attending meetings is the opportunity to take advantage of the various wet labs available. Having the guidance of experienced surgeons through my first attempts at the big bubble technique for a deep anterior lamellar keratoplasty and picking up real-time pearls for phakic IOL insertion at an annual ophthalmology meeting greatly enhanced my learning process.
Videos are invaluable to the visual learner.

BY JONATHAN SOLOMON, MD
One thing we ophthalmologists learn once we are in practice is that we never stop learning. I like to pull from all the available resources for my continuing education and have made a habit of annually visiting a different colleague in the OR as part of a mini sabbatical. When I am not listening to SiriusXM Doctor Radio or Rosetta Stone, I am listening to Audio-Digest Ophthalmology on the way to the office. On my lunch break, I typically have a sandwich with a slice of the American Academy of Ophthalmology’s Focal Points module, which has been a mainstay of the office (and a favorite of my father’s generation).
Today, we have several ways to access educational resources, which allows us to choose to learn in the manner that is best for us. Because I have always been a visual learner, explanations of a surgical technique on paper have never made a lot of sense to me. Even with still photographs, illustrations, figures, or sketches, I was always left wanting clarification. I would read the articles and imagine how the hand was maneuvering or how a needle was being passed. Now, video digests and online videos are my go-to for surgical developments and advances.
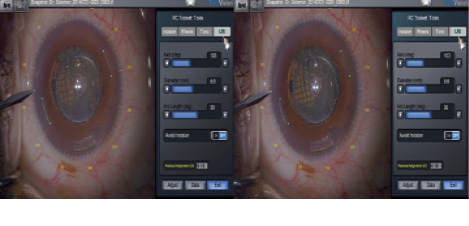
Figure. Three-dimensional video allows for better knowledge transfer of surgical techniques
PEER-REVIEWED LITERATURE IN PRINT
I still prefer to follow the peer-reviewed literature in print. My first stop is frequently the Journal of Refractive Surgery, which offers succinct cogent clinical studies, and I also peruse the Journal of Cataract and Refractive Surgery’s (JCRS) technique section with the online video accompaniment. The management of complex cases is always fascinating. In a recent issue of JCRS, for example, I read with interest the article on the use of femtosecond laser technology to treat posterior polar cataracts. I pay particular attention to the genesis of a technique and what advantages the authors believe the technique confers.
Alternatively, if I want to view a particular technique that I may have heard discussed at a large meeting or seen reviewed in CRST or AOC, I can review the video resources associated with those publications, EyetubeOD and Eyetube.net. Online, I type in a few key words like Descemet membrane endothelial keratoplasty and get a listing of what is available. As I access high-quality collections of similar videos and peruse techniques, I often find myself heading in a different direction due to the novelty of the cases posted. This stream of consciousness I experience when viewing cataloged videos regularly leads me down a path of new ideas.
ADVICE FROM COLLEAGUES
It is not uncommon for me to call a few colleagues who maintain fastidious catalogs of surgical cases for advice. A surgical dilemma or my preparation for a complicated case might begin with a quick email to my friends. Colleagues in the Vanguard Ophthalmology Society, Cornea External Disease and Refractive Surgery, and American Society of Progressive Enterprising Surgeons coalition often provide sage advice in times of need and an informal dialogue to facilitate the climb up a challenging learning curve. For instance, when I used the Verus ophthalmic caliper (Mile High Ophthalmics) for the first time, I was able to review surgical cases online at the manufacturer’s website (www.milehighophthalmics.com). Then, I emailed a few experienced colleagues, who forwarded to me a few of their own videos for a final bit of prep work. In return, I later provided my first few cases to the group for critique.
CONCLUSION
I am excited about the advent of three-dimensional cameras and televisions and the role they play in my ongoing education (Figure). We ophthalmologists can now share surgical procedures in a format that provides unprecedented image quality and depth of focus and tremendous potential for stress-free learning from the comfort of our homes.
Plug into colleagues and the digital world.

BY GARY WöRTZ, MD
Ophthalmology is an ever-advancing field with a culture that promotes and rewards innovation. We surgeons are always on the lookout for the next new procedure and ways to improve our techniques for better outcomes in the meantime. After leaving residency and fellowship, however, we are left to find ways to continuously improve our surgical approach. Thankfully, there are many great resources for gathering and spreading good ideas.
GETTING PLUGGED IN
In my opinion, every surgeon needs a community of other surgeons that he or she trusts. Whether it is a city or state organization or a national group like American-European College of Ophthalmic Surgery, American College of Eye Surgeons/SEE, American Society of Cataract and Refractive Surgery, or the like, having people you trust to bounce ideas off makes all the difference in the world. For doctors looking to get plugged into a wider network, the national meetings provide a tremendously powerful opportunity for friendship and the transfer of information.
For example, my journey began at the Kiawah Eye Meeting where I had the good fortune to meet William B. Trattler, MD, and George O. Waring IV, MD. We started sharing ideas, and before the weekend was over, I had met many other key ophthalmologists who were more than happy to offer their perspectives on the current state of our profession. That led to my attending the American-European College of Ophthalmic Surgery Deer Valley meeting, where I met even more of the same type of forward-thinking, innovative surgeons. I still remember arriving at the St. Regis for the cocktail reception, where I ran into Jeffrey Whitman, MD. We started talking about IOL exchanges, and he shared a tip with me that forever changed my approach. I had never read it in a journal and was not taught the approach in residency. It seems that being in the right place at the right time provided me with an amazing opportunity to learn. For learning to take place, however, egos need to be put aside, and we must be willing to ask for help and receive advice. Since that conversation with Jeff, I have shared the technique with others. In fact, I just had a local doctor ask me for some advice on a challenging IOL exchange this week, and I passed along what I had learned. So, having a group of ophthalmologists that I trust and being willing to both learn and educate make the process really enjoyable for all involved.

The author at MillennialEYE’s inaugural meeting in Austin, Texas, with George O. Waring IV, MD, William B. Trattler, MD, and Paul Kang, MD.
ONLINE/REMOTE RESOURCES
Having a network is key, but it certainly is not the only way to learn new information. Reading the monthly trade journals like CRST is a great way to keep up with new innovations. I look through each issue, read the articles that interest me, and even copy the articles that I feel need to be shared with my partners or other doctors. The peer-reviewed literature is also a very powerful tool that should not be overlooked, but I typically use these resources to evaluate the efficacy of my practice patterns through evidence-based medicine, rather than for the incorporation of new techniques.
Online resources such as Eyetube.net provide an extensive library of videos showcasing surgical techniques. This is an important tool when I am considering adding a new procedure to my repertoire. Watching other surgeons in action and seeing the differences in approaches can be very helpful. A wonderful blend of trade journal-style information and multimedia resources can be found in the MillennialEYE app that is available to download free from the Apple Store. This bimonthly publication provides a fresh approach to sharing information, with links to surgical videos and discussions about what works in the real world.
Soon, there will be a new option for learning surgical pearls that I hope will incorporate all of these important factors into a simple format. Thanks to BMC, publisher of CRST, I will be hosting a monthly podcast called “Ophthalmology off the Grid.” The goal is to have honest conversations with other ophthalmologists about the procedures and techniques that have really helped them in their practices. As mentioned previously, it can be the cocktail reception-type of conversations that change practice patterns, and I hope to channel this style of frank discussion into a new media channel. The podcast will be informal, fun, and perhaps irreverent at times, but most importantly, it will be educational. We are all busy, and podcasts are a great way to learn while traveling or commuting to work.
CONCLUSION
Being a physician requires a commitment to being a lifetime learner. Thankfully, we have tremendous access to great resources from which to learn. Learning new techniques can be intimidating, and I believe our specialty has a disproportionate amount of talented and willing teachers who are more than happy to share their experiences. For all of these reasons, I am proud to be practicing in this exciting era. n
William F. Wiley, MD
• in practice at the Cleveland Eye Clinic in Ohio
• assistant clinical professor of ophthalmology at University Hospitals/Case Western Reserve University, Cleveland
• (440) 526-1974; drwiley@clevelandeyeclinic.com; Twitter @wiley2020
Elizabeth Yeu, MD
• assistant professor of ophthalmology, Eastern Virginia Medical School, Ghent, Virginia
• partner specializing in cornea, cataract, and refractive surgery at Virginia Eye Consultants, Norfolk, Virginia
• (757) 662-2200; eyeu@vec2020.com
• financial disclosure: consultant to Alcon
Jonathan Solomon, MD
• surgical/refractive director, Solomon Eye Physicians and Surgeons, Greenbelt and Bowie, Maryland, and McLean, Virginia
• jdsolomon@hotmail.com
• Financial disclosure: None acknowledged
Gary Wörtz, MD
• cataract and refractive surgeon at Commonwealth Eye Surgery in Lexington, Kentucky
• founder and chief medical officer of Omega Ophthalmics
• drwortz@omegalens.com

